You might also like
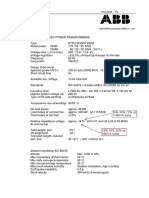
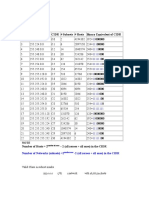
- ABB 3wdg TRAFO Data SheetDocument2 pagesABB 3wdg TRAFO Data SheetKunik SwaroopNo ratings yet
- Anatomic VariantsDocument12 pagesAnatomic VariantssaadNo ratings yet
- Acetabular Labral Tears Diagnosis RepairDocument13 pagesAcetabular Labral Tears Diagnosis RepairwladjaNo ratings yet
- Hip Scope AnchorDocument9 pagesHip Scope AnchorMarcelo Wiltemburg AlvesNo ratings yet
- Arce 2013Document11 pagesArce 2013Fillipe AgraNo ratings yet
- Currentconceptsof Femoroacetabular Impingement: Aria Ghaffari,, Ivan Davis,, Troy Storey,, Michael MoserDocument18 pagesCurrentconceptsof Femoroacetabular Impingement: Aria Ghaffari,, Ivan Davis,, Troy Storey,, Michael MosertanyasisNo ratings yet
- Intervalo de Los Rotadores PDFDocument10 pagesIntervalo de Los Rotadores PDFdiegovirusNo ratings yet
- Cornea2006LacrimalGland AnatomyhistopathologyDocument9 pagesCornea2006LacrimalGland AnatomyhistopathologyRochnald PigaiNo ratings yet
- Femoral Acetabular Impingement: RadiographyDocument9 pagesFemoral Acetabular Impingement: Radiography杨钦杰No ratings yet
- The Calcar Femorale: A New Perspective: or Thopaedic Surger yDocument9 pagesThe Calcar Femorale: A New Perspective: or Thopaedic Surger ycalinNo ratings yet
- Diagnosis and Management of Sacral Spine Fractures: J Bone Joint Surg AmDocument12 pagesDiagnosis and Management of Sacral Spine Fractures: J Bone Joint Surg AmAmanda Cuastumal AguirreNo ratings yet
- Labrum PosteriorDocument13 pagesLabrum PosteriorMustika Ainun FadhilaNo ratings yet
- Femoral Shaft Fractures in AdultsDocument12 pagesFemoral Shaft Fractures in AdultsDiego BellingNo ratings yet
- OUtcome After Limted or Extensive BursectomyDocument8 pagesOUtcome After Limted or Extensive BursectomySeno adipNo ratings yet
- An Anatomic Arthroscopic Description of The Hip Capsular Ligaments For The Hip ArthroscopistDocument9 pagesAn Anatomic Arthroscopic Description of The Hip Capsular Ligaments For The Hip Arthroscopistxekar59382No ratings yet
- Biomechanical and Anatomical Consequences of Carpal Tunnel ReleaseDocument9 pagesBiomechanical and Anatomical Consequences of Carpal Tunnel ReleaseSylvia GraceNo ratings yet
- Dvorak1988 2Document10 pagesDvorak1988 2mona khosraviNo ratings yet
- Wrist Anatomy and Biomechanics: American Society For Surgery of The Hand.)Document9 pagesWrist Anatomy and Biomechanics: American Society For Surgery of The Hand.)Roberto Alonso Lopez SantanaNo ratings yet
- Corona Mortis: An Anatomical Study With Clinical Implications in Approaches To The Pelvis and AcetabulumDocument7 pagesCorona Mortis: An Anatomical Study With Clinical Implications in Approaches To The Pelvis and Acetabulummartina marinoNo ratings yet
- Magnetic Resonance Imaging of The HipDocument11 pagesMagnetic Resonance Imaging of The HipsaadNo ratings yet
- Khan 2012Document7 pagesKhan 2012Daniel PredaNo ratings yet
- Pao 2003Document12 pagesPao 2003Milton Ricardo de Medeiros FernandesNo ratings yet
- Fractures of The Talus Current ConceptsDocument10 pagesFractures of The Talus Current ConceptsBalsam TeineNo ratings yet
- 0 1 The Pathophysiology of Shoulder Instability 2800953368Document8 pages0 1 The Pathophysiology of Shoulder Instability 2800953368César ArveláezNo ratings yet
- M O Intro6Document19 pagesM O Intro6DANIEL FRANCISCO ACOSTA ACOSTANo ratings yet
- Sonopathology 2Document9 pagesSonopathology 2Ivette M. Carroll D.No ratings yet
- Rsa FlapDocument11 pagesRsa Flapdhivya kannanNo ratings yet
- 2012 - Ramo Pulmonar Na Artéria Celíaca em CãoDocument3 pages2012 - Ramo Pulmonar Na Artéria Celíaca em CãoMagnoDosSantosRozaNo ratings yet
- Through: Hanflig, Schlosberg, M.D.TDocument4 pagesThrough: Hanflig, Schlosberg, M.D.Trich sitaNo ratings yet
- ISMT 12 - Day 383 - Vito - Lumbopelvic Fixation TechniquesDocument18 pagesISMT 12 - Day 383 - Vito - Lumbopelvic Fixation TechniquesVito MasagusNo ratings yet
- Ijav 10 056-058Document3 pagesIjav 10 056-058Rehan AsadNo ratings yet
- Harry Et Al-1997-Clinical AnatomyDocument3 pagesHarry Et Al-1997-Clinical AnatomyJuan José CabezasNo ratings yet
- Diagnosis and Management of The Painful Shoulder (1) - Part 1 Clinical Anatomy and PathomechanicsDocument20 pagesDiagnosis and Management of The Painful Shoulder (1) - Part 1 Clinical Anatomy and PathomechanicsFabian LuisNo ratings yet
- Puntos Anatomicos para Estabilización de Luxació Sacroiliaca en GatoDocument6 pagesPuntos Anatomicos para Estabilización de Luxació Sacroiliaca en Gatowilfredo ferrel muñozNo ratings yet
- The Effect of Calcar Femoral Neck Plating On VascuDocument7 pagesThe Effect of Calcar Femoral Neck Plating On VascuHoàng LongNo ratings yet
- Hypothesis of Human Penile Anatomy, Erection Hemodynamics and Their Clinical ApplicationsDocument10 pagesHypothesis of Human Penile Anatomy, Erection Hemodynamics and Their Clinical ApplicationsPeter69No ratings yet
- The Wiltse para Spinal Approach To The LumbarDocument6 pagesThe Wiltse para Spinal Approach To The LumbarJoao Domingos Carneiro LeaoNo ratings yet
- Pinzamiento AcetabulofemoralDocument9 pagesPinzamiento AcetabulofemoraldanypauloNo ratings yet
- Alue Devies, 2019.imaging of The Foot andDocument8 pagesAlue Devies, 2019.imaging of The Foot andFarhan RendyNo ratings yet
- Caudal Anesthesia - NYSORADocument27 pagesCaudal Anesthesia - NYSORApradeep daniel100% (1)
- Nonoperative and Operative Management ofDocument12 pagesNonoperative and Operative Management ofVladislav KotovNo ratings yet
- 9 10 Art 1780260219Document5 pages9 10 Art 1780260219canhtung1989No ratings yet
- Anatomy of CF Lig. 2020Document5 pagesAnatomy of CF Lig. 2020Ahmed MortadaNo ratings yet
- Biomechanical Factors in Rotator Cuff PathologyDocument5 pagesBiomechanical Factors in Rotator Cuff PathologyYa ChenNo ratings yet
- Anatomi EyelidDocument9 pagesAnatomi EyelidFelyana GunawanNo ratings yet
- The Insertional Footprint of The Rotator Cuff: An Anatomic StudyDocument8 pagesThe Insertional Footprint of The Rotator Cuff: An Anatomic StudySandro RolimNo ratings yet
- Parosteal Lipoma of Proximal Radius A Rare Case ReDocument4 pagesParosteal Lipoma of Proximal Radius A Rare Case ReKRISHNA19651No ratings yet
- Castling 2015Document3 pagesCastling 2015Jonathan PanchiNo ratings yet
- Hip AssessDocument6 pagesHip AssessAhmed SalmanNo ratings yet
- Anterior Achromioplasty For The Chronic Impingement Syndrome in The ShoulderDocument1 pageAnterior Achromioplasty For The Chronic Impingement Syndrome in The ShoulderJefferson James Dos SantosNo ratings yet
- Hip Anatomical Variations As A Possible Onset of Coxarthrosis in Young Patients 2012 Journal of BiomechanicsDocument1 pageHip Anatomical Variations As A Possible Onset of Coxarthrosis in Young Patients 2012 Journal of BiomechanicssilviaNo ratings yet
- Fraser MoodieDocument11 pagesFraser MoodieWiindaNo ratings yet
- Waitayawinyu 2007Document13 pagesWaitayawinyu 2007Milton Ricardo de Medeiros FernandesNo ratings yet
- The Anatomy of The Anterior Cruciate Ligament and Its Relevance To The Technique of ReconstructionDocument7 pagesThe Anatomy of The Anterior Cruciate Ligament and Its Relevance To The Technique of ReconstructionMetin HakkanNo ratings yet
- Osseous Fixation Pathways in Pelvic and Acetabular Fracture Surgery Osteology, Radiology and Clinical Applications 2011Document8 pagesOsseous Fixation Pathways in Pelvic and Acetabular Fracture Surgery Osteology, Radiology and Clinical Applications 2011Gonzalo JimenezNo ratings yet
- AnatomyandBiomechanicsoftheNativeand ReconstructedAnteriorCruciateLigamen PDFDocument8 pagesAnatomyandBiomechanicsoftheNativeand ReconstructedAnteriorCruciateLigamen PDFRoman PopescuNo ratings yet
- Innervation of The Acromioclavicular Joint by The Suprascapular NerveDocument6 pagesInnervation of The Acromioclavicular Joint by The Suprascapular NervemitroisergiuNo ratings yet
- Journal of Orthopaedics: B.T. Pushpa, Siddharth N. Aiyer, Muhil Kannan, Anupama Maheswaran, S. RajasekaranDocument2 pagesJournal of Orthopaedics: B.T. Pushpa, Siddharth N. Aiyer, Muhil Kannan, Anupama Maheswaran, S. RajasekaranmohNo ratings yet
- The "Ligamentization" Process in Anterior Cruciate Ligament ReconstructionDocument9 pagesThe "Ligamentization" Process in Anterior Cruciate Ligament Reconstructionmarcelogascon.oNo ratings yet
- Anatomy of The Anterior Cruciate Ligament With.9Document13 pagesAnatomy of The Anterior Cruciate Ligament With.9Metin HakkanNo ratings yet
- Management of Intraoperative Graft Related.3Document9 pagesManagement of Intraoperative Graft Related.3cooperorthopaedicsNo ratings yet
- Stepwise Safe Access in Hip Arthroscopy in The.1Document9 pagesStepwise Safe Access in Hip Arthroscopy in The.1cooperorthopaedicsNo ratings yet
- Nonsurgical Versus Surgical Management Of.3Document8 pagesNonsurgical Versus Surgical Management Of.3cooperorthopaedicsNo ratings yet
- Cartilage Regeneration.7Document9 pagesCartilage Regeneration.7cooperorthopaedicsNo ratings yet
- COA SAEQuestionLibrary 2Document104 pagesCOA SAEQuestionLibrary 2cooperorthopaedicsNo ratings yet
- Musculoskeletal Effects of Cancer and Cancer.5Document13 pagesMusculoskeletal Effects of Cancer and Cancer.5cooperorthopaedicsNo ratings yet
- Principles of Amputation Surgery, Prosthetics, And.7Document12 pagesPrinciples of Amputation Surgery, Prosthetics, And.7cooperorthopaedicsNo ratings yet
- Unplanned Resection of Sarcoma.3Document10 pagesUnplanned Resection of Sarcoma.3cooperorthopaedicsNo ratings yet
- Sports 2021Document78 pagesSports 2021cooperorthopaedicsNo ratings yet
- X Is Surgical Resection of The Primary Site.17Document12 pagesX Is Surgical Resection of The Primary Site.17cooperorthopaedicsNo ratings yet
- X - The Natural History of Benign Bone Tumors of The Extremities in Asymptomatic ChildrenDocument6 pagesX - The Natural History of Benign Bone Tumors of The Extremities in Asymptomatic ChildrencooperorthopaedicsNo ratings yet
- Fellows Reading List - 2017-18Document8 pagesFellows Reading List - 2017-18cooperorthopaedicsNo ratings yet
- S6 Upper Cervical Spine TraumaDocument82 pagesS6 Upper Cervical Spine TraumacooperorthopaedicsNo ratings yet
- Journal Pre-Proof: Arthroscopy: The Journal of Arthroscopic and Related SurgeryDocument29 pagesJournal Pre-Proof: Arthroscopy: The Journal of Arthroscopic and Related SurgerycooperorthopaedicsNo ratings yet
- PIIS1058274622009053Document6 pagesPIIS1058274622009053cooperorthopaedicsNo ratings yet
- Next Generation Sequencing Results Require Higher.1239Document8 pagesNext Generation Sequencing Results Require Higher.1239cooperorthopaedicsNo ratings yet
- Joc60156 2451 2459Document9 pagesJoc60156 2451 2459cooperorthopaedicsNo ratings yet
- CFSS Checklist For SchoolsDocument9 pagesCFSS Checklist For SchoolsSharie ArellanoNo ratings yet
- Export Meaning, Significance and Methods in IndiaDocument9 pagesExport Meaning, Significance and Methods in IndiaPayal AroraNo ratings yet
- DLL - Science 3 - Q1 - W8Document3 pagesDLL - Science 3 - Q1 - W8Jefferson Beralde100% (2)
- Unit-4-Methods of TrainingDocument40 pagesUnit-4-Methods of TrainingManoj KumarNo ratings yet
- Science Lines 1Document68 pagesScience Lines 1Mark Lloyd ColomaNo ratings yet
- SAD WireframeDocument1 pageSAD WireframeRhene LlonaNo ratings yet
- Unit 2 Lesson 2 Honors ApplyDocument3 pagesUnit 2 Lesson 2 Honors ApplyJohn SynchrosNo ratings yet
- Niir Complete Book On Rubber Processing Compounding Technology With Machinery Details 2nd Revised EditionDocument13 pagesNiir Complete Book On Rubber Processing Compounding Technology With Machinery Details 2nd Revised EditionMarcoNo ratings yet
- Reflection On Written AssignmentDocument3 pagesReflection On Written Assignmentapi-302720012No ratings yet
- Workover and Analysis Well ProblemsDocument61 pagesWorkover and Analysis Well ProblemsTeddy GeovanieNo ratings yet
- Tender Spec in Arabic - Ar.en - Ar.enDocument37 pagesTender Spec in Arabic - Ar.en - Ar.enMohamad ChaudhariNo ratings yet
- SUBNETTINGDocument4 pagesSUBNETTINGEmmanuel AduKissieduNo ratings yet
- 7914 13992 1 SM PDFDocument22 pages7914 13992 1 SM PDFsuratiniraiNo ratings yet
- Research Methods in Education: B. Ed (1.5 YEAR)Document287 pagesResearch Methods in Education: B. Ed (1.5 YEAR)HiraNo ratings yet
- Residential Land - Plot For Sale in Bharati Nagar Dharwad - 267 Sq. YardDocument6 pagesResidential Land - Plot For Sale in Bharati Nagar Dharwad - 267 Sq. Yardshakeelbaigt3No ratings yet
- Enable TDE in Oracle GG Classic ModeDocument5 pagesEnable TDE in Oracle GG Classic ModeAvinash SinghNo ratings yet
- Can Fant PDFDocument47 pagesCan Fant PDFFernanda CarvalhoNo ratings yet
- Manual Event Corporate TownhallDocument14 pagesManual Event Corporate TownhallDiva Bella Permata - D3 KeperawatanNo ratings yet
- Cookery 10 LASQ1Document6 pagesCookery 10 LASQ1Erich Niña AyoNo ratings yet
- Oracles RMCSDocument34 pagesOracles RMCSsharas77No ratings yet
- Move by Move - PetrosianDocument144 pagesMove by Move - Petrosianleonilsonsv50% (2)
- Definition of LiberalizationDocument5 pagesDefinition of LiberalizationFiles DownloadNo ratings yet
- Lab 1 CircuitDocument8 pagesLab 1 Circuitapi-610008741No ratings yet
- Rufino, Hillary - Eng 302-The Rise of Greek DramaDocument3 pagesRufino, Hillary - Eng 302-The Rise of Greek DramaHillary RufinoNo ratings yet
- الماجستير المهنى فى العلوم الاكتوارية PDFDocument2 pagesالماجستير المهنى فى العلوم الاكتوارية PDFOmran KingNo ratings yet
- How Astrologer Differentiate Love Marriage Vs Only Love Relationship - by Akashvaani - MediumDocument6 pagesHow Astrologer Differentiate Love Marriage Vs Only Love Relationship - by Akashvaani - MediumDamien LockkeNo ratings yet
- Calculating Cable Fault RatingsDocument1 pageCalculating Cable Fault Ratingswaqas_a_shaikh4348No ratings yet
- Reversible Reactions & Dynamic Equilibrium 3 QPDocument18 pagesReversible Reactions & Dynamic Equilibrium 3 QPSam GreenNo ratings yet
- Cost-to-Serve Model (CTS) : CIPS Procurement TopicDocument6 pagesCost-to-Serve Model (CTS) : CIPS Procurement TopicRoshanNo ratings yet