You might also like
- Safety and Reference: Owner'S ManualDocument84 pagesSafety and Reference: Owner'S ManualjpmcorpNo ratings yet
- Opioid Agonists and AntagonistsDocument5 pagesOpioid Agonists and AntagonistsCas BuNo ratings yet
- Ovaries & AdnexaeDocument124 pagesOvaries & AdnexaeabafzNo ratings yet
- Urology Physical Examination For BUPSDocument22 pagesUrology Physical Examination For BUPSLuki ErtandriNo ratings yet
- Hematuria, (Blood in Urine) A Simple Guide to The Condition, Related Diseases And Use in Diagnosis of DiseasesFrom EverandHematuria, (Blood in Urine) A Simple Guide to The Condition, Related Diseases And Use in Diagnosis of DiseasesRating: 5 out of 5 stars5/5 (2)
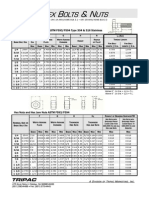
- Imperial Bolts Nuts & WashersDocument7 pagesImperial Bolts Nuts & WashersstugwynneNo ratings yet
- Imaging Tractus UrinaryDocument94 pagesImaging Tractus UrinaryJuan Ortega PutraNo ratings yet
- HydronephrosisDocument43 pagesHydronephrosisjessyNo ratings yet
- Module 6 - Benign Gynecologic TumorsDocument9 pagesModule 6 - Benign Gynecologic TumorsRenz Francis SasaNo ratings yet
- Imaging in Genitourinary SystemDocument77 pagesImaging in Genitourinary SystemIrvan R. Loho100% (1)
- Applied Eco - Q4 - M4Document12 pagesApplied Eco - Q4 - M4bernadette domoloan100% (2)
- Male GU ExamDocument5 pagesMale GU ExamOmar Farid ElgebalyNo ratings yet
- HematuriaDocument86 pagesHematuriaMohamad Arif MustaphaNo ratings yet
- Emergency in Urology - Edit241021Document76 pagesEmergency in Urology - Edit241021Alverina Ode Nifaki100% (1)
- Culture Media and MethodsDocument49 pagesCulture Media and Methodscj bariasNo ratings yet
- Scrotal SwellingDocument63 pagesScrotal SwellingTommysNo ratings yet
- Ultrasound of Srotal Emergency in PediatricDocument53 pagesUltrasound of Srotal Emergency in PediatricIsti Iryan PriantiNo ratings yet
- Technical ProposalDocument4 pagesTechnical ProposalolescootNo ratings yet
- Uterovaginal ProlapseDocument52 pagesUterovaginal ProlapseAmeera K Khan75% (4)
- Imaging in Genitourinary System - 17 Agustus 2013 - by Robby HermawanDocument80 pagesImaging in Genitourinary System - 17 Agustus 2013 - by Robby HermawanFitria Dewi LestariNo ratings yet
- Congenital Anomalies of Ureter BladderDocument17 pagesCongenital Anomalies of Ureter BladderAfiq SabriNo ratings yet
- ZF 6wg310Document192 pagesZF 6wg310Tomasz BedrunkaNo ratings yet
- Urology MCQs PDFDocument13 pagesUrology MCQs PDFendiNo ratings yet
- Set 4Document19 pagesSet 4Dick Morgan FerrerNo ratings yet
- Imperforate AnusDocument51 pagesImperforate AnusBheru LalNo ratings yet
- Albaflow JETDocument12 pagesAlbaflow JETTrinhTruong100% (1)
- The Kidneys & Ureters - NEWDocument12 pagesThe Kidneys & Ureters - NEWnasir iqbalNo ratings yet
- Uro PedsooDocument9 pagesUro Pedsoomotasem.med120No ratings yet
- Pediatric Urological Disorders: Professor Adel Al-HunayanDocument44 pagesPediatric Urological Disorders: Professor Adel Al-Hunayanmarina_shawkyNo ratings yet
- Mip Dunnick Ch5 - The RetroperitoneumDocument60 pagesMip Dunnick Ch5 - The Retroperitoneummark padulloNo ratings yet
- 03 US Alteraciones Congenitas RiñonDocument7 pages03 US Alteraciones Congenitas RiñonDonaldo ReleyNo ratings yet
- Kidney & Urinary Tract USDocument62 pagesKidney & Urinary Tract USBayarbaatar BoldNo ratings yet
- Testicular SwellingDocument66 pagesTesticular SwellingbrnardNo ratings yet
- Introduction in UrologyDocument69 pagesIntroduction in UrologyKaram SaadNo ratings yet
- Imaging PadaDocument77 pagesImaging PadaNaja HasnandaNo ratings yet
- Hydronephrosis OutlineDocument13 pagesHydronephrosis OutlineSarah Sy-SantosNo ratings yet
- Torsio TestisDocument19 pagesTorsio TestisRandy HarrisNo ratings yet
- Physical Examination of The Genitourinary TractDocument3 pagesPhysical Examination of The Genitourinary Tractmary_chdhry100% (1)
- App Novi Lia (Edit)Document42 pagesApp Novi Lia (Edit)MeganitaNo ratings yet
- What Is Epispadias?: Bladder ExstrophyDocument3 pagesWhat Is Epispadias?: Bladder ExstrophylailiafjNo ratings yet
- Examination of A StomaDocument3 pagesExamination of A StomaChloe100% (1)
- Chapter 9Document11 pagesChapter 9hanniaitiel69No ratings yet
- Emergency Urology Non TraumaticDocument51 pagesEmergency Urology Non TraumaticJeremi SetiawanNo ratings yet
- Tractus UrinariusDocument23 pagesTractus UrinariusYaleswari Hayu PertiwiNo ratings yet
- HydronephrosisDocument11 pagesHydronephrosis黃昱睿No ratings yet
- Sites: - Ureteric CalculiDocument16 pagesSites: - Ureteric CalculiBersisa chalchisaNo ratings yet
- EpispadiasisDocument12 pagesEpispadiasisvishnuNo ratings yet
- Scrotal Swelling: 'By Kasyeba Sowedi Mbchb-IiiDocument57 pagesScrotal Swelling: 'By Kasyeba Sowedi Mbchb-IiiNinaNo ratings yet
- Renal SurgeryDocument62 pagesRenal Surgeryalvin salvationNo ratings yet
- Epispadiasis (Paediatrics)Document3 pagesEpispadiasis (Paediatrics)Linumol JosephNo ratings yet
- Acute Scrotal Pain - 2Document52 pagesAcute Scrotal Pain - 2surajit chandNo ratings yet
- b9 PKM 2 Urinary Retention Dr. Christian Ronald Tanggo Sp.uDocument63 pagesb9 PKM 2 Urinary Retention Dr. Christian Ronald Tanggo Sp.uDaud ParluhutanNo ratings yet
- اسايمنتDocument57 pagesاسايمنتMall HiNo ratings yet
- History Taking and Physical Examination in Urologic PatientsDocument25 pagesHistory Taking and Physical Examination in Urologic PatientsAdebisiNo ratings yet
- CYSTOSTOMYDocument60 pagesCYSTOSTOMYOepil KirickNo ratings yet
- IVU - DR Juned A AnsariDocument50 pagesIVU - DR Juned A AnsariJuned A AnsariNo ratings yet
- Urinary RetentionDocument64 pagesUrinary RetentionAntonioIndraTNo ratings yet
- Anorectal Malformatio N: Dr. O. Sankoh M.D. House Officer Pediatric SurgeryDocument123 pagesAnorectal Malformatio N: Dr. O. Sankoh M.D. House Officer Pediatric SurgeryMohamed KamaraNo ratings yet
- Gastrointestinal System DiseasesDocument6 pagesGastrointestinal System DiseasesHazel ConjeNo ratings yet
- Anatomy and Blood Supply of AppendixDocument30 pagesAnatomy and Blood Supply of AppendixForam PatelNo ratings yet
- Radiology of The Urinary SystemDocument78 pagesRadiology of The Urinary Systemapi-19916399No ratings yet
- Acute Urinary Retention: Ronald TanggoDocument63 pagesAcute Urinary Retention: Ronald TanggoKalista ApriyaniNo ratings yet
- Urological Physical ExaminationDocument5 pagesUrological Physical ExaminationSirajum MuneeraNo ratings yet
- Investigations of The Urinary TractDocument26 pagesInvestigations of The Urinary TractOnkar SinghNo ratings yet
- Categories of Malformations: Anomalies of Number, Volume and Structure Ascent, Form and Fusion, Rotation andDocument3 pagesCategories of Malformations: Anomalies of Number, Volume and Structure Ascent, Form and Fusion, Rotation andÁngel Parra CominoNo ratings yet
- Male Genitalia ExaminationDocument6 pagesMale Genitalia ExaminationParthik PatelNo ratings yet
- Kub IvpDocument46 pagesKub IvpBryJos tiongsonNo ratings yet
- Anorectal Malformation New 2024Document34 pagesAnorectal Malformation New 2024Urologi RSunudNo ratings yet
- Urethrolithiasis - EditDocument37 pagesUrethrolithiasis - EditShabrina Sari MedinaNo ratings yet
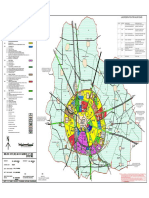
- Jhajjar Master PlanDocument1 pageJhajjar Master PlanMayank AhujaNo ratings yet
- Solar Powered Field Server and Aerator Development For Lake PalakpakinDocument9 pagesSolar Powered Field Server and Aerator Development For Lake Palakpakindragh meh downNo ratings yet
- Mount Pinatubo Case StudyDocument8 pagesMount Pinatubo Case StudyafmoanrbdNo ratings yet
- CH 6 Combustion and Flames Qs AnsDocument4 pagesCH 6 Combustion and Flames Qs AnsAditya Kumar MishraNo ratings yet
- ABC ClassificationDocument11 pagesABC ClassificationJUan Banquez GarciaNo ratings yet
- 2.3 Monitor Unit: - MU-201CR (20 Inch LCD) - MU-231CR (23 Inch LCD)Document3 pages2.3 Monitor Unit: - MU-201CR (20 Inch LCD) - MU-231CR (23 Inch LCD)PhuocTranThienNo ratings yet
- Relación de Tablas SAPDocument29 pagesRelación de Tablas SAPduran_jxcsNo ratings yet
- Private Student DormitoriesDocument4 pagesPrivate Student DormitoriesHimadri DasNo ratings yet
- Data Coll Action of ResortDocument62 pagesData Coll Action of ResortLakshmiRaviChanduKolusu0% (1)
- Dipin Damodaran's: ClassesDocument17 pagesDipin Damodaran's: ClassesAmit KakkarNo ratings yet
- Exure Determination Determination ChromatographyDocument3 pagesExure Determination Determination ChromatographyDennis Limaymanta YupanquiNo ratings yet
- Chap02 Decision Modelling Using SpreadsheetDocument36 pagesChap02 Decision Modelling Using SpreadsheetamritaNo ratings yet
- Tmecc 0410Document7 pagesTmecc 0410Karen BenteoNo ratings yet
- Breaking Waves: A New Concept For Pile Supported Skirt BreakwatersDocument22 pagesBreaking Waves: A New Concept For Pile Supported Skirt BreakwaterspsuvarnasNo ratings yet
- Improvement of Voltage Profile Through The Optimal Placement of FACTS Using L-Index MethodDocument5 pagesImprovement of Voltage Profile Through The Optimal Placement of FACTS Using L-Index MethodRavishankar KankaleNo ratings yet
- Concept of Tensors Deformation of A Body Stress Equilibrium Equations Constitutive Equations Principles From Work and Energy Homework ReferencesDocument19 pagesConcept of Tensors Deformation of A Body Stress Equilibrium Equations Constitutive Equations Principles From Work and Energy Homework Referencess2rajiNo ratings yet
- Hitachi ABB Power Grids - EconiQ-1Document1 pageHitachi ABB Power Grids - EconiQ-1Ciprian RhamnusiaNo ratings yet
- Idoc - Pub Ic4l2t1to8akeyDocument1 pageIdoc - Pub Ic4l2t1to8akeySantiago MadridNo ratings yet
- CE 107: Introduction To Civil and Environmental EngineeringDocument26 pagesCE 107: Introduction To Civil and Environmental Engineeringnahid rahmanNo ratings yet
- Microlog & Microlog Plus User Guide: Eighth Edition First Print Printed in February 2005Document211 pagesMicrolog & Microlog Plus User Guide: Eighth Edition First Print Printed in February 2005ecaph2440% (1)
- Repair SMPS PC (For Example, JNC SY-300ATX) - Repair and Renovation - Blogs ElectronicsDocument7 pagesRepair SMPS PC (For Example, JNC SY-300ATX) - Repair and Renovation - Blogs ElectronicsaladinthewizardNo ratings yet