You might also like
- Lesson Plan On Placenta PraeviaDocument14 pagesLesson Plan On Placenta PraeviaSanthu Su67% (6)
- Lesson Plan On Uterine Abnormality and Displacement: B.SC Nursing StudentsDocument20 pagesLesson Plan On Uterine Abnormality and Displacement: B.SC Nursing StudentsKinjal VasavaNo ratings yet
- Placental ExaminationDocument12 pagesPlacental ExaminationNidhi Sharma100% (7)
- OBSTETRICS - 1.05 Preconception and Prenatal Care (Dr. Famador) - 1Document7 pagesOBSTETRICS - 1.05 Preconception and Prenatal Care (Dr. Famador) - 1Lchg KrvyNo ratings yet
- Infant Perception: from Sensation to Cognition: Basic Visual ProcessesFrom EverandInfant Perception: from Sensation to Cognition: Basic Visual ProcessesLeslie B. CohenNo ratings yet
- OBG Theses TopicsDocument22 pagesOBG Theses TopicsNavya Sanjeeva Reddy100% (4)
- Stages of LaborDocument23 pagesStages of LaborPortia Dulce Toquero100% (5)
- Uterine Prolapse Lession PlanDocument10 pagesUterine Prolapse Lession PlanRaj JadhavNo ratings yet
- Abortion Lesssion PlanDocument37 pagesAbortion Lesssion PlanRaj JadhavNo ratings yet
- VESICULAR NEW Lession PlanDocument18 pagesVESICULAR NEW Lession PlanRaj JadhavNo ratings yet
- Lesson Plan On Subinvolution of UterusDocument8 pagesLesson Plan On Subinvolution of UterusMansiNo ratings yet
- APH Lession PlanDocument20 pagesAPH Lession PlanRaj JadhavNo ratings yet
- Unit-Plan: Submitted By: Ms - Prerna SharmaDocument4 pagesUnit-Plan: Submitted By: Ms - Prerna SharmaPrernaSharma67% (3)
- Uterine Rupture and Cervical TearDocument16 pagesUterine Rupture and Cervical Tearsangita patil0% (1)
- L P APHDocument11 pagesL P APHmoni khatkarNo ratings yet
- Vaginal ExaminationDocument16 pagesVaginal ExaminationVarna MohanNo ratings yet
- Antepartum HemorrhageDocument7 pagesAntepartum HemorrhageGood Life.No ratings yet
- BS.C Nursing 3 Year Child Health Nursing Unit-PlanDocument9 pagesBS.C Nursing 3 Year Child Health Nursing Unit-Planshubham vermaNo ratings yet
- Katherine CaseDocument8 pagesKatherine CaseCeejay PardilloNo ratings yet
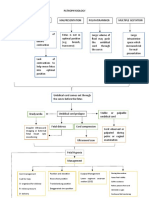
- Pathophysio (Ucp)Document2 pagesPathophysio (Ucp)Rachelle Joy AsuncionNo ratings yet
- Midwifery and Obstetrical Nursing: Course DescriptionDocument36 pagesMidwifery and Obstetrical Nursing: Course DescriptionrenjiniNo ratings yet
- Lession Plan On 1st Stage of LabourDocument15 pagesLession Plan On 1st Stage of LabourRaj JadhavNo ratings yet
- Intrautrian Growth RetarDocument11 pagesIntrautrian Growth RetarJyoti Prem Uttam100% (3)
- Lession Plan On Physiology of 3rd Stage of LabourDocument11 pagesLession Plan On Physiology of 3rd Stage of LabourRaj JadhavNo ratings yet
- Antenatal LessonplanDocument7 pagesAntenatal Lessonplanpemalhamu188No ratings yet
- Lakshmi Micro TeachingDocument20 pagesLakshmi Micro Teachingduddela lakshmi100% (1)
- OB - Operative Vaginal Delivery (AJB)Document5 pagesOB - Operative Vaginal Delivery (AJB)Darren Mae MosadaNo ratings yet
- LESSON PLAN FOR PLACENTA EXAMINATION NHDHFDocument10 pagesLESSON PLAN FOR PLACENTA EXAMINATION NHDHFjrkedridgemwanakalandoNo ratings yet
- Partograph NotessssDocument17 pagesPartograph NotessssSunil KumarNo ratings yet
- Iit and ValueDocument21 pagesIit and ValueKartik GuptaNo ratings yet
- Lesson Plan On Induction of LaborDocument16 pagesLesson Plan On Induction of LaborPriyanka YadavNo ratings yet
- Lesson Plan EpisiotomyDocument12 pagesLesson Plan Episiotomyshivani das100% (2)
- Teaching Practice GeneticsDocument23 pagesTeaching Practice GeneticsAsha jiluNo ratings yet
- Client Initials: Medical Diagnosis: Cephalopelvic Disproportion Eu DEFINITION: The RelationshipDocument2 pagesClient Initials: Medical Diagnosis: Cephalopelvic Disproportion Eu DEFINITION: The RelationshipLyssa Monique67% (3)
- LP Antenatal ExaminationDocument7 pagesLP Antenatal ExaminationManisha ThakurNo ratings yet
- Leopold's ManeuverDocument6 pagesLeopold's ManeuverPrecious Shaira AbagNo ratings yet
- All India Institute of Medical Sciences, Jodhpur College of Nursing Lesson Plan ON TopicDocument12 pagesAll India Institute of Medical Sciences, Jodhpur College of Nursing Lesson Plan ON TopicFarheen khanNo ratings yet
- Lesson Plan of Fetal MeasureDocument5 pagesLesson Plan of Fetal Measuresuman guptaNo ratings yet
- Self Introduction:: SR. NO Time Specific Objectives Content Teacher'S Activity Stdent'S Activity A.V. Aids EvaluationDocument11 pagesSelf Introduction:: SR. NO Time Specific Objectives Content Teacher'S Activity Stdent'S Activity A.V. Aids EvaluationJuhi Johnson Jadhav83% (6)
- Lesson Plan SynopsisDocument19 pagesLesson Plan Synopsisshivani dasNo ratings yet
- Ru LRDR1Document3 pagesRu LRDR1JadeNo ratings yet
- Lesson Plan On Neonatal ConvulsionDocument19 pagesLesson Plan On Neonatal ConvulsionASHISH KUMAR YADAV100% (1)
- OB TemplateDocument1 pageOB TemplateryfullanteNo ratings yet
- Destructive SurgriesDocument19 pagesDestructive Surgriesshivani dasNo ratings yet
- Lesson Plan Placenta PreviaDocument18 pagesLesson Plan Placenta Previasaroj hayatNo ratings yet
- Breast Examination 2Document7 pagesBreast Examination 2Miriward ZimbaNo ratings yet
- Growth Flourish Master Challenge Further Challenge Animal Sexual ReproductionDocument2 pagesGrowth Flourish Master Challenge Further Challenge Animal Sexual Reproductionakshyta gantanNo ratings yet
- Abnormal Labor, Dystocia IIDocument9 pagesAbnormal Labor, Dystocia IIIke RilleraNo ratings yet
- BBSC Midwifery N Obstetrical NsgTheory 060210 23082012 1438Document21 pagesBBSC Midwifery N Obstetrical NsgTheory 060210 23082012 1438Amol SakhareNo ratings yet
- B. Sc. 3 Year PDFDocument92 pagesB. Sc. 3 Year PDFSanthosh.S.UNo ratings yet
- Fourth Year B SC Nursing Obstetric and Gynaecological Nursing Obstetric NursingDocument35 pagesFourth Year B SC Nursing Obstetric and Gynaecological Nursing Obstetric Nursingsandeepv080% (1)
- Ew BSC Course PlanDocument21 pagesEw BSC Course PlanBHUKYA USHARANINo ratings yet
- Constriction Ring Pathological RingDocument13 pagesConstriction Ring Pathological RingVarna MohanNo ratings yet
- MALPRESENTATIONDocument13 pagesMALPRESENTATIONLady Jane CaguladaNo ratings yet
- A Neurological Study of Newborn Infants: Clinics in Developmental Medicine, No. 28From EverandA Neurological Study of Newborn Infants: Clinics in Developmental Medicine, No. 28No ratings yet
- Every Child Can Fly: An Early Childhood Educator's Guide to InclusionFrom EverandEvery Child Can Fly: An Early Childhood Educator's Guide to InclusionNo ratings yet
- Development and Evolution of Brain Size: Behavioral ImplicationsFrom EverandDevelopment and Evolution of Brain Size: Behavioral ImplicationsMartine HahnNo ratings yet
- Development of Perception: Psychobiological PerspectivesFrom EverandDevelopment of Perception: Psychobiological PerspectivesRichard AslinNo ratings yet
- Pmsma Reporting Performa Up To 10 June 2017Document1 pagePmsma Reporting Performa Up To 10 June 2017jaswinderkaur081974No ratings yet
- Healthy Timing and Spacing of Pregnancy (HTSP)Document5 pagesHealthy Timing and Spacing of Pregnancy (HTSP)mnmrznNo ratings yet
- Partus LamaDocument11 pagesPartus LamaSulis SipinNo ratings yet
- Common Terminologies in ObstetricsDocument4 pagesCommon Terminologies in ObstetricsDolly Jane JavierNo ratings yet
- 15-Article Text-153-1-10-20210918Document14 pages15-Article Text-153-1-10-20210918Bayu Fitria MaharaniNo ratings yet
- Post Partum DeathDocument12 pagesPost Partum DeathFerzada SajiranNo ratings yet
- COMPONENTS OF LABOR - 5PsDocument5 pagesCOMPONENTS OF LABOR - 5PslumpiaNo ratings yet
- Occipito Posterior PositionDocument52 pagesOccipito Posterior PositionVijith.V.kumar100% (3)
- Health Promotion "Exclusive Breast Milk"Document3 pagesHealth Promotion "Exclusive Breast Milk"Linda SaputriNo ratings yet
- Placental ExaminationDocument5 pagesPlacental ExaminationReema Akberali nooraniNo ratings yet
- Youth in Action: Preventing Teenage PregnancyDocument41 pagesYouth in Action: Preventing Teenage PregnancyDeleon AizaNo ratings yet
- NUR 1025 Exam 1 NotesDocument3 pagesNUR 1025 Exam 1 NotesfpltdcNo ratings yet
- Obg Qus Set4Document24 pagesObg Qus Set4Imraan KhanNo ratings yet
- Bemonc: Basic Emergency Obstetric and Newborn CareDocument32 pagesBemonc: Basic Emergency Obstetric and Newborn CareIzhra MargateNo ratings yet
- PPIUDDocument16 pagesPPIUDmusicwizardNo ratings yet
- Early Pregnancy TestDocument13 pagesEarly Pregnancy TestLucian MihuNo ratings yet
- BibliographyDocument6 pagesBibliographyPiyush DuttaNo ratings yet
- Maternal and Foetal Outcome of Single Dose Spinal Analgesia For Labour PainsDocument3 pagesMaternal and Foetal Outcome of Single Dose Spinal Analgesia For Labour PainsGurnaman SinghNo ratings yet
- Mechanisms of LaborDocument16 pagesMechanisms of LaborRyan Robert V. Ventolero100% (1)
- Inter-Hospital Variations in Labor Induction and OutcomesDocument9 pagesInter-Hospital Variations in Labor Induction and OutcomesStéphanieNo ratings yet
- Anna Liza R. Alfonso RN, RM, ManDocument13 pagesAnna Liza R. Alfonso RN, RM, ManAnnaAlfonsoNo ratings yet
- Common Causes of Dysfunctional Labor:: DystociaDocument8 pagesCommon Causes of Dysfunctional Labor:: DystociaAngelo ArabejoNo ratings yet
- DPR - Head Duty Sateve 24.12.22Document11 pagesDPR - Head Duty Sateve 24.12.22bobbyrianto2210No ratings yet
- Maternal Cosmetics Use During Pregnancy and Risks of Adverse Outcomes A Prospective Cohort StudyDocument8 pagesMaternal Cosmetics Use During Pregnancy and Risks of Adverse Outcomes A Prospective Cohort StudyLeni SafitriNo ratings yet
- Medical Care 1 PDFDocument2 pagesMedical Care 1 PDFDen LacambraNo ratings yet
- By Debra BettsDocument6 pagesBy Debra BettsAudrygodwyn100% (3)
- 51 EpisiotomyDocument21 pages51 Episiotomydr_asaleh100% (2)
- Prolonged LaborDocument13 pagesProlonged Laborsujinaranamagar18No ratings yet