You might also like
- Passive Voice Transformations PDFDocument4 pagesPassive Voice Transformations PDFInvitado51895256% (9)
- Aon Care GHS Claim FormDocument5 pagesAon Care GHS Claim FormGelson Herrera0% (5)
- Hotel Incident ReportDocument2 pagesHotel Incident ReportApirinmu100% (7)
- 22-23 AP Language CompsitionDocument60 pages22-23 AP Language CompsitionFatoma AlnassirNo ratings yet
- Incident Report FormDocument3 pagesIncident Report FormUbuntu Linux100% (8)
- IFE Study Materials Through LearnProDocument2 pagesIFE Study Materials Through LearnPromohammad waqas33% (3)
- 03 For Supplier Iresource & ISDP Operation PDFDocument18 pages03 For Supplier Iresource & ISDP Operation PDFBelkheir SalimNo ratings yet
- Midterm C ETF 2016Document4 pagesMidterm C ETF 2016GausNo ratings yet
- Form GDocument2 pagesForm GAAK AlAin100% (1)
- NP-NEOM-OSH-Form 05 Incident Notification FormDocument2 pagesNP-NEOM-OSH-Form 05 Incident Notification FormyasirNo ratings yet
- Serious OSH Incident Investigation Report - V3.0 EnglishDocument5 pagesSerious OSH Incident Investigation Report - V3.0 EnglishkapilNo ratings yet
- MMF136 Accident Investigation ReportDocument3 pagesMMF136 Accident Investigation ReportMurali KrishnaNo ratings yet
- Incident Report TemplateDocument3 pagesIncident Report Templateapi-412577219No ratings yet
- Accident - Incident Report - FormDocument3 pagesAccident - Incident Report - FormdanyNo ratings yet
- Accident Report FormDocument5 pagesAccident Report Formyenni mirandaNo ratings yet
- Sample Incident Investigation FormsDocument5 pagesSample Incident Investigation FormsshahbazchafekarNo ratings yet
- Form G2 - Non-Serious OSH Incident Investigation Report - V3.0 EnglishDocument5 pagesForm G2 - Non-Serious OSH Incident Investigation Report - V3.0 Englishraja50% (2)
- Report of Unusul Incident - Workplace ViolenceDocument2 pagesReport of Unusul Incident - Workplace ViolenceEyob DIANANo ratings yet
- Fire Alarm Incident Report 02 April 2024Document3 pagesFire Alarm Incident Report 02 April 2024Mohsin RazaNo ratings yet
- First Aid Accident Form WPADocument2 pagesFirst Aid Accident Form WPAshaibaz chafekarNo ratings yet
- HSSE World Incident Report Form 1Document10 pagesHSSE World Incident Report Form 1Rayhan FalahNo ratings yet
- Incident Report FormDocument3 pagesIncident Report FormAvril CervantesNo ratings yet
- Module 11 - Brittany BruceDocument4 pagesModule 11 - Brittany Bruceapi-532087532No ratings yet
- Gemini Logistics PTY LTD: Incident Report FormDocument3 pagesGemini Logistics PTY LTD: Incident Report FormMac MNo ratings yet
- Form 23, Incident InvestigationDocument4 pagesForm 23, Incident Investigationathul subashNo ratings yet
- 10.2 Incident Report A - ESEC-HSE-F-10.2 Rev.02Document2 pages10.2 Incident Report A - ESEC-HSE-F-10.2 Rev.02zaigham naqviNo ratings yet
- Incident Report FormDocument3 pagesIncident Report Formapi-375638716No ratings yet
- Incident and Accident Form: UI-61917-PGCC-HSSE-IAF 3.1Document4 pagesIncident and Accident Form: UI-61917-PGCC-HSSE-IAF 3.1benNo ratings yet
- Accident or Dangerous Incident Report FormDocument4 pagesAccident or Dangerous Incident Report FormFNo ratings yet
- Liability Claim Form: Particulars of Insured (Company I Individual)Document3 pagesLiability Claim Form: Particulars of Insured (Company I Individual)Bounna PhoumalavongNo ratings yet
- Appendix 2. ALDAR Projects OSH Incident Investigation ReportDocument8 pagesAppendix 2. ALDAR Projects OSH Incident Investigation Reporterwin.tamayo1982No ratings yet
- Incident ReportDocument2 pagesIncident ReportJawed KhanNo ratings yet
- Accident-Incident Report FormDocument1 pageAccident-Incident Report FormKrishna SrikanthNo ratings yet
- Organisation Details: Details of The Consumer Affected by This IncidentDocument3 pagesOrganisation Details: Details of The Consumer Affected by This Incidentmitchellbird83No ratings yet
- Employee Medical Incident ReportDocument1 pageEmployee Medical Incident ReportAiswarya SukumarNo ratings yet
- Incident Investigation Report FormDocument7 pagesIncident Investigation Report FormAlexis MillsNo ratings yet
- SW - Ci - Const - Fillable CsirDocument10 pagesSW - Ci - Const - Fillable CsirJaycee Bareng PagadorNo ratings yet
- Accident Investigation ReportDocument3 pagesAccident Investigation ReportKhan Mohammad Mahmud HasanNo ratings yet
- Incident FormDocument2 pagesIncident FormCINQO HSENo ratings yet
- QR-ADM-1010 Incident Report TPSMIDocument17 pagesQR-ADM-1010 Incident Report TPSMIHR SundiaNo ratings yet
- Ico Nis Reporting FormDocument7 pagesIco Nis Reporting FormMichael nandoNo ratings yet
- Accident Form Template: Developed byDocument5 pagesAccident Form Template: Developed byEcinaj CabahugNo ratings yet
- Accident Form Template: Developed byDocument5 pagesAccident Form Template: Developed byj.andry. dprNo ratings yet
- Assg Incidentreportform 20180122 Ah102Document2 pagesAssg Incidentreportform 20180122 Ah102api-393314541No ratings yet
- Report of An Injury or Dangerous Occurrence: Part A Part CDocument2 pagesReport of An Injury or Dangerous Occurrence: Part A Part CVeronica Navarro CorbiNo ratings yet
- Accident Investigation Report: Investigator's InformationDocument2 pagesAccident Investigation Report: Investigator's InformationJack PNo ratings yet
- QHSE Manual: Document NameDocument3 pagesQHSE Manual: Document NameFarhanNo ratings yet
- Construction INCIDENT ReportDocument2 pagesConstruction INCIDENT ReportmontusinghbokaroNo ratings yet
- RMoE Incident Report TemplateDocument1 pageRMoE Incident Report TemplateJovy Dela Merced GarciaNo ratings yet
- Incident FormDocument5 pagesIncident FormMurtadda Mohammed100% (1)
- Standard Incident Report FormDocument2 pagesStandard Incident Report FormEssie MohammedNo ratings yet
- Accident/Incident Report Section 1: Details of Person Making This ReportDocument2 pagesAccident/Incident Report Section 1: Details of Person Making This ReportAbdul RafeequeNo ratings yet
- Lamp Sesi 8.2 Investigasi SCATDocument2 pagesLamp Sesi 8.2 Investigasi SCATaab kanayaNo ratings yet
- HSE-F-NEOM-008 - Final Incident-Accident ReportDocument4 pagesHSE-F-NEOM-008 - Final Incident-Accident ReportAhmed MohamedNo ratings yet
- Incident ReportDocument2 pagesIncident ReportLeila LaouitiNo ratings yet
- Incident Report FormDocument2 pagesIncident Report FormMuhammad Ibad AlamNo ratings yet
- Incident Report Form: RPSG-IMS-F-24 Accident and Investigation Form 5ADocument2 pagesIncident Report Form: RPSG-IMS-F-24 Accident and Investigation Form 5ARocky Bis100% (1)
- Accident Incident Investigaton ReportDocument4 pagesAccident Incident Investigaton ReportPlanning EngineerNo ratings yet
- CheiDocument3 pagesCheiapi-389332081No ratings yet
- Incident and Hazard Report Form - v1.0Document4 pagesIncident and Hazard Report Form - v1.0Vraj ShahNo ratings yet
- HSE Incident Report RevDocument2 pagesHSE Incident Report RevBee100% (1)
- Incident Report Form: RPSG-IMS-F-24 Accident and Investigation Form 5ADocument2 pagesIncident Report Form: RPSG-IMS-F-24 Accident and Investigation Form 5ARocky BisNo ratings yet
- Safety Incident Report FormDocument3 pagesSafety Incident Report FormDiego MatillaNo ratings yet
- Disaster Dollars: Financial Preparation and Recovery for Towns, Businesses, Farms, and IndividualsFrom EverandDisaster Dollars: Financial Preparation and Recovery for Towns, Businesses, Farms, and IndividualsNo ratings yet
- 05register - Work Permit RegisterDocument1 page05register - Work Permit Registermohammad waqasNo ratings yet
- 7 Thioflex 600 PDFDocument12 pages7 Thioflex 600 PDFmohammad waqasNo ratings yet
- PPE 2 Head ProtectionDocument7 pagesPPE 2 Head Protectionmohammad waqasNo ratings yet
- WeldingDocument102 pagesWeldingmohammad waqasNo ratings yet
- WPR Updated Instructor NotesDocument22 pagesWPR Updated Instructor Notesmohammad waqas100% (1)
- Fire Safety: Unit 2, Activity 2Document10 pagesFire Safety: Unit 2, Activity 2mohammad waqasNo ratings yet
- Marhaba FlyerDocument8 pagesMarhaba Flyermohammad waqasNo ratings yet
- Fall Protection PDFDocument13 pagesFall Protection PDFmohammad waqasNo ratings yet
- Saudi Labour Law 090406111356 Phpapp02Document52 pagesSaudi Labour Law 090406111356 Phpapp02Sudhi SudhiNo ratings yet
- Confined SpaceDocument1 pageConfined Spacemohammad waqasNo ratings yet
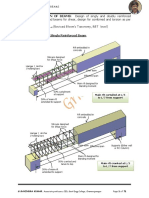
- Beams, Design of Flanged Beams For Shear, Design For Combined and Torsion As Per IS - 456. 10 Hours L and L (Revised Bloom's Taxonomy, RBT Level)Document71 pagesBeams, Design of Flanged Beams For Shear, Design For Combined and Torsion As Per IS - 456. 10 Hours L and L (Revised Bloom's Taxonomy, RBT Level)Viji NpNo ratings yet
- Format: This Exam Has 25 Questions. There Are Multiple Choice, Matching, Fill in The Blank, andDocument13 pagesFormat: This Exam Has 25 Questions. There Are Multiple Choice, Matching, Fill in The Blank, andAna M SierraNo ratings yet
- Dustin Nguyen - Google SearchDocument6 pagesDustin Nguyen - Google SearchTertuliano RodriguesNo ratings yet
- Faculty Member, Himachal Institute of Life Sciences: Ashok KumarDocument12 pagesFaculty Member, Himachal Institute of Life Sciences: Ashok KumarasokumrNo ratings yet
- Friday MyplateDocument2 pagesFriday Myplateapi-653788186No ratings yet
- Glassman Idea GenerationDocument70 pagesGlassman Idea GenerationkabeerbiswasNo ratings yet
- Accomplishment Distinguished Extra-Ordinary: SakuntalaandDocument2 pagesAccomplishment Distinguished Extra-Ordinary: SakuntalaandJaseena YasminNo ratings yet
- DecentralizationDocument8 pagesDecentralizationMrito ManobNo ratings yet
- Acid Related DisordersDocument56 pagesAcid Related DisordersDr-Firas Nayf Al-ThawabiaNo ratings yet
- CHO-Sem III-Module I-IPM Industrial Psychology-July-AugDocument5 pagesCHO-Sem III-Module I-IPM Industrial Psychology-July-AugDigvijay ChauhanNo ratings yet
- Tattoo HomeworkDocument6 pagesTattoo Homeworkersesjv5No ratings yet
- Krok 2 2012-2019Document59 pagesKrok 2 2012-2019Donya GholamiNo ratings yet
- Abbott V Alcaraz DigestDocument4 pagesAbbott V Alcaraz DigestcattaczNo ratings yet
- Healing With Roses WorkshopDocument35 pagesHealing With Roses WorkshopScribdTranslationsNo ratings yet
- Aims & Objectives of Creation of Pakistan: Taimoor Muzaffar GondalDocument17 pagesAims & Objectives of Creation of Pakistan: Taimoor Muzaffar GondalSana EjazNo ratings yet
- Nutrient Requirements of GoatsDocument16 pagesNutrient Requirements of GoatsHanneza JoaquinoNo ratings yet
- Art 1110 Gallery Critique Essay Rough DraftDocument3 pagesArt 1110 Gallery Critique Essay Rough Draftapi-458754996No ratings yet
- Arnold On Teaching MathematicsDocument9 pagesArnold On Teaching MathematicsmehdiukNo ratings yet
- P.1 Term IIIDocument32 pagesP.1 Term IIImpaabe167No ratings yet
- Lista AuspiciadoresDocument2 pagesLista AuspiciadoresWanda MendezNo ratings yet
- The Concept of Romanticism IDocument24 pagesThe Concept of Romanticism ISiddhartha PratapaNo ratings yet
- Kom CTDocument3 pagesKom CTUmesh Kumar GanjirNo ratings yet
- Holding CoDocument35 pagesHolding Coshilpi raniNo ratings yet
- Karl Marx Historical MaterialismDocument11 pagesKarl Marx Historical MaterialismAarush RajputNo ratings yet
- C. Ayyappan and V.C. Harris Spectral SpeechDocument6 pagesC. Ayyappan and V.C. Harris Spectral SpeechNasrullah Mambrol100% (1)
- Pain Management in The Emergency: Dr. Prathiba Prasad Emergency Physician Masafi HospitalDocument50 pagesPain Management in The Emergency: Dr. Prathiba Prasad Emergency Physician Masafi HospitalPrathiba PrassaddNo ratings yet