You might also like
- Foundations of Airport Economics and FinanceFrom EverandFoundations of Airport Economics and FinanceRating: 5 out of 5 stars5/5 (1)
- Direct Property & Casualty Insurance Carrier Revenues World Summary: Market Values & Financials by CountryFrom EverandDirect Property & Casualty Insurance Carrier Revenues World Summary: Market Values & Financials by CountryNo ratings yet
- University Hospitals Form 5500 Year 2010 Employee Benefit PlanDocument68 pagesUniversity Hospitals Form 5500 Year 2010 Employee Benefit PlanJames LindonNo ratings yet
- Kaiser Supplemental Savings and Retirement Plan Annual Report Form 5500Document37 pagesKaiser Supplemental Savings and Retirement Plan Annual Report Form 5500James LindonNo ratings yet
- Charles SchwabDocument45 pagesCharles SchwabThe Washington PostNo ratings yet
- CostcoDocument41 pagesCostcoThe Washington PostNo ratings yet
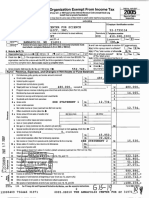
- (Jjo Jmt4 - : Return of Organization Exempt From Income TaxDocument18 pages(Jjo Jmt4 - : Return of Organization Exempt From Income Taxcmf8926No ratings yet
- NFL Retirement Board 2013 Filing Form 5500Document252 pagesNFL Retirement Board 2013 Filing Form 5500Jeff NixonNo ratings yet
- LJ LJ: Return of Organization Exempt From Income TaxDocument20 pagesLJ LJ: Return of Organization Exempt From Income Taxcmf8926No ratings yet
- US Internal Revenue Service: f5500st - 1999Document2 pagesUS Internal Revenue Service: f5500st - 1999IRSNo ratings yet
- Form No. 15G: Area Code AO Type Range Code Ao NoDocument2 pagesForm No. 15G: Area Code AO Type Range Code Ao NoRanjan ManoNo ratings yet
- 2012 Building Intl Bridges (03!28!2013)Document17 pages2012 Building Intl Bridges (03!28!2013)Jk McCreaNo ratings yet
- U.S. Information Return Trust Accumulation of Charitable AmountsDocument4 pagesU.S. Information Return Trust Accumulation of Charitable AmountspdizypdizyNo ratings yet
- Donors Capital Fund541934032 2007 048EED01SearchableDocument28 pagesDonors Capital Fund541934032 2007 048EED01Searchablecmf8926No ratings yet
- FreedomWorks Foundation 521526916 2006 0317E2DASearchableDocument25 pagesFreedomWorks Foundation 521526916 2006 0317E2DASearchablecmf8926No ratings yet
- Audit of General Insurance CompaniesDocument20 pagesAudit of General Insurance CompaniesZiniaKhanNo ratings yet
- Institute For Liberty 202641983 2008 076b44aeDocument4 pagesInstitute For Liberty 202641983 2008 076b44aecmf8926No ratings yet
- Return of Private Foundation or Section 49 A7 @) (11 Nonexempt Charitable TrustDocument15 pagesReturn of Private Foundation or Section 49 A7 @) (11 Nonexempt Charitable TrustalavifoundationNo ratings yet
- Claude R Lambe Charitable Foundation 480935563 2011 08d6a523Document24 pagesClaude R Lambe Charitable Foundation 480935563 2011 08d6a523cmf8926No ratings yet
- Schedule R (Form 941)Document3 pagesSchedule R (Form 941)Francis Wolfgang UrbanNo ratings yet
- 2010 Form 990 For President and Fellows of Harvard CollegeDocument254 pages2010 Form 990 For President and Fellows of Harvard CollegeresponsibleharvardNo ratings yet
- IRS Reporting Requirements Under The Affordable Care Act Is Your Business Ready?Document8 pagesIRS Reporting Requirements Under The Affordable Care Act Is Your Business Ready?api-284589375No ratings yet
- $e ., - .22 - May, 2al9: of Af of 42Document12 pages$e ., - .22 - May, 2al9: of Af of 42Ekansh AroraNo ratings yet
- FormcDocument20 pagesFormc420deepakNo ratings yet
- All Withholding Is A Gift!Document8 pagesAll Withholding Is A Gift!Tom Harkins100% (2)
- 2009 Form 990 For Harvard Management CompanyDocument55 pages2009 Form 990 For Harvard Management CompanyresponsibleharvardNo ratings yet
- Final Audit - Insurance Audit Notes PDFDocument9 pagesFinal Audit - Insurance Audit Notes PDFBhavin Nilesh PandyaNo ratings yet
- Cfi - Fy2004 - F990Document37 pagesCfi - Fy2004 - F990Didi RemezNo ratings yet
- FTG Irs Form 990 2006Document19 pagesFTG Irs Form 990 2006L. A. PatersonNo ratings yet
- Return of Organization Exempt From Income Tax: IX) IX)Document21 pagesReturn of Organization Exempt From Income Tax: IX) IX)cmf8926No ratings yet
- India Sudar TaxFile 2005-06Document7 pagesIndia Sudar TaxFile 2005-06India Sudar Educational and Charitable Trust100% (1)
- Esi Form 5 WordDocument3 pagesEsi Form 5 Wordpummy124No ratings yet
- ICIRR Money and OrganizationsDocument73 pagesICIRR Money and OrganizationsOmar Jonathan Pérez MoralesNo ratings yet
- Return of Private Foundation or Sectio N 9a7 @L (11 Nonexempt Charitable TrustDocument15 pagesReturn of Private Foundation or Sectio N 9a7 @L (11 Nonexempt Charitable TrustalavifoundationNo ratings yet
- US Internal Revenue Service: A-04-38Document3 pagesUS Internal Revenue Service: A-04-38IRSNo ratings yet
- AFS 2020 Annual ReportDocument178 pagesAFS 2020 Annual ReportN.a. M. TandayagNo ratings yet
- Barbara and Barrie Seid Foundation 363342443 2011 08e875b6searchableDocument22 pagesBarbara and Barrie Seid Foundation 363342443 2011 08e875b6searchablecmf8926No ratings yet
- Form 990-P F: Return of Private FoundationDocument26 pagesForm 990-P F: Return of Private FoundationFund for Democratic CommunitiesNo ratings yet
- SECForm 17-A - As AmendedDocument7 pagesSECForm 17-A - As AmendedJon PinedaNo ratings yet
- General Instructions For Certain Information Returns: RemindersDocument19 pagesGeneral Instructions For Certain Information Returns: Remindersmstinson1No ratings yet
- Mcq-Pgbp-Ito Exam-2020Document9 pagesMcq-Pgbp-Ito Exam-2020Durgadevi BaskaranNo ratings yet
- GSRG 405 PT 1Document17 pagesGSRG 405 PT 1LaLa BanksNo ratings yet
- Ls 208Document1 pageLs 208El CapitánNo ratings yet
- Bidding DocumentsDocument15 pagesBidding DocumentsRhyann MosendeNo ratings yet
- Threshold Foundation 2008 990Document41 pagesThreshold Foundation 2008 990TheSceneOfTheCrimeNo ratings yet
- Securities and Exchange Commission (SEC) - Formn-CsrDocument8 pagesSecurities and Exchange Commission (SEC) - Formn-CsrhighfinanceNo ratings yet
- SRG1801Document7 pagesSRG1801Abel BellNo ratings yet
- Accenture 10KDocument168 pagesAccenture 10KSumit GuptaNo ratings yet
- Form No.16: Part ADocument3 pagesForm No.16: Part AYogesh DhekaleNo ratings yet
- FreedomWorks Inc 521349353 2005 0263603DSearchableDocument18 pagesFreedomWorks Inc 521349353 2005 0263603DSearchablecmf8926No ratings yet
- ASML 2012 Annual AccountsDocument150 pagesASML 2012 Annual Accountsjasper laarmansNo ratings yet
- SPT PPH BDN 2009 English OrtaxDocument39 pagesSPT PPH BDN 2009 English Ortaxanon_265770590No ratings yet
- Bid Data Sheet: 1.1 The Procuring Entity IsDocument7 pagesBid Data Sheet: 1.1 The Procuring Entity IsrheyNo ratings yet
- PSU Right To Know Report 2011Document71 pagesPSU Right To Know Report 2011OpDeathEatersUSNo ratings yet
- The Bilderberg Group Tax Returns 2010Document23 pagesThe Bilderberg Group Tax Returns 2010Jonathan Robert Kraus (OutofMudProductions)No ratings yet
- Nidhi-Amendment 2019-20Document12 pagesNidhi-Amendment 2019-20Manoj KumarNo ratings yet
- Reinsurance Carrier Revenues World Summary: Market Values & Financials by CountryFrom EverandReinsurance Carrier Revenues World Summary: Market Values & Financials by CountryNo ratings yet
- Miscellaneous Intermediation Revenues World Summary: Market Values & Financials by CountryFrom EverandMiscellaneous Intermediation Revenues World Summary: Market Values & Financials by CountryNo ratings yet
- 09.06.2018 StarmanDocument7 pages09.06.2018 StarmanJames LindonNo ratings yet
- 09.14.2018 NgohDocument9 pages09.14.2018 NgohJames LindonNo ratings yet
- Anderson ComplaintDocument15 pagesAnderson ComplaintBasseemNo ratings yet
- State Of: Steven W. Schierholt, Esq. Executive Director John R. GaDocument6 pagesState Of: Steven W. Schierholt, Esq. Executive Director John R. GaJames LindonNo ratings yet
- 10.10.2018 GomezDocument5 pages10.10.2018 GomezJames LindonNo ratings yet
- Sc-,:iegi?5: in The Matter Of: CASE NO. 2016-1909 License No. 02-1339450Document6 pagesSc-,:iegi?5: in The Matter Of: CASE NO. 2016-1909 License No. 02-1339450James LindonNo ratings yet
- State Of: PendingDocument7 pagesState Of: PendingJames LindonNo ratings yet
- 1.3.18 Ohio Board of Pharmacy Notice of Opportunity For Hearing James LindonDocument8 pages1.3.18 Ohio Board of Pharmacy Notice of Opportunity For Hearing James LindonJames LindonNo ratings yet
- 09.06.2018 Pamela ApplegateDocument6 pages09.06.2018 Pamela ApplegateJames LindonNo ratings yet
- 09.26.2018 LottDocument6 pages09.26.2018 LottJames LindonNo ratings yet
- 10.02.2018 MascioDocument6 pages10.02.2018 MascioJames LindonNo ratings yet
- 8.23.18 Better Living Clinic AkronDocument5 pages8.23.18 Better Living Clinic AkronJames LindonNo ratings yet
- James Lindon Attorney, Ph.D. 35104 Saddle Creek Avon, Ohio 44011-4907Document1 pageJames Lindon Attorney, Ph.D. 35104 Saddle Creek Avon, Ohio 44011-4907James LindonNo ratings yet
- Robert Garrity Prison RecordDocument1 pageRobert Garrity Prison RecordJames LindonNo ratings yet
- 1.25.18 Ohio Board of Pharmacy Notice of Opportunity For Hearing James LindonDocument13 pages1.25.18 Ohio Board of Pharmacy Notice of Opportunity For Hearing James LindonJames LindonNo ratings yet
- Attachment Formulary 2500Document46 pagesAttachment Formulary 2500James LindonNo ratings yet
- LCBA's 79th President, Andrea Kryszak, Takes Over: Summer, 2015 Volume 10, Issue 3Document21 pagesLCBA's 79th President, Andrea Kryszak, Takes Over: Summer, 2015 Volume 10, Issue 3James LindonNo ratings yet
- Lorain County Government DirectoryDocument53 pagesLorain County Government DirectoryJames LindonNo ratings yet
- Certification of Micro Entity StatusDocument2 pagesCertification of Micro Entity StatusJames LindonNo ratings yet
- COURTESY Reception Good MannersDocument1 pageCOURTESY Reception Good MannersGulzina ZhumashevaNo ratings yet
- Adjective & VerbsDocument3 pagesAdjective & VerbsDennis BerkNo ratings yet
- Virtual Assets Act, 2022Document18 pagesVirtual Assets Act, 2022Rapulu UdohNo ratings yet
- HRMDocument118 pagesHRMKarthic KasiliaNo ratings yet
- Individual Career Plan: DIRECTIONS: Answer The Following Questions in Paragraph Form (3-4 Sentences) Per QuestionDocument2 pagesIndividual Career Plan: DIRECTIONS: Answer The Following Questions in Paragraph Form (3-4 Sentences) Per Questionapi-526813290No ratings yet
- WHO Guidelines For Drinking Water: Parameters Standard Limits As Per WHO Guidelines (MG/L)Document3 pagesWHO Guidelines For Drinking Water: Parameters Standard Limits As Per WHO Guidelines (MG/L)114912No ratings yet
- 1Document3 pages1Stook01701No ratings yet
- ETAP Power Station ErrorDocument5 pagesETAP Power Station ErroryogacruiseNo ratings yet
- Google Tools: Reggie Luther Tracsoft, Inc. 706-568-4133Document23 pagesGoogle Tools: Reggie Luther Tracsoft, Inc. 706-568-4133nbaghrechaNo ratings yet
- Project Management TY BSC ITDocument57 pagesProject Management TY BSC ITdarshan130275% (12)
- Odisha State Museum-1Document26 pagesOdisha State Museum-1ajitkpatnaikNo ratings yet
- To Find Fatty Material of Different Soap SamplesDocument17 pagesTo Find Fatty Material of Different Soap SamplesRohan Singh0% (2)
- Data Asimilasi Untuk PemulaDocument24 pagesData Asimilasi Untuk PemulaSii Olog-olog PlonkNo ratings yet
- 5 Minute Pediatric ConsultDocument5 pages5 Minute Pediatric Consultajescool0% (4)
- Case Study - Kelompok 2Document5 pagesCase Study - Kelompok 2elida wenNo ratings yet
- Chapter 4 - Basic ProbabilityDocument37 pagesChapter 4 - Basic Probabilitynadya shafirahNo ratings yet
- Haier in India Building Presence in A Mass Market Beyond ChinaDocument14 pagesHaier in India Building Presence in A Mass Market Beyond ChinaGaurav Sharma100% (1)
- Santu BabaDocument2 pagesSantu Babaamveryhot0950% (2)
- Introduction To DifferentiationDocument10 pagesIntroduction To DifferentiationaurennosNo ratings yet
- Top 100 Chemical CompaniesDocument11 pagesTop 100 Chemical Companiestawhide_islamicNo ratings yet
- Specifications (018-001) : WarningDocument6 pagesSpecifications (018-001) : WarningRómulo Simón Lizarraga LeónNo ratings yet
- Segregation in CastingDocument17 pagesSegregation in CastingAsmaa Smsm Abdallh78% (9)
- Student Management SystemDocument232 pagesStudent Management Systemslu_mangal73% (37)
- Bandhan Neft Rtgs FormDocument2 pagesBandhan Neft Rtgs FormMohit Goyal50% (4)
- Lab Report SBK Sem 3 (Priscilla Tuyang)Document6 pagesLab Report SBK Sem 3 (Priscilla Tuyang)Priscilla Tuyang100% (1)
- Contoh Discussion Text Tentang HomeworkDocument8 pagesContoh Discussion Text Tentang Homeworkg3p35rs6100% (1)
- Automatic Gearbox ZF 4HP 20Document40 pagesAutomatic Gearbox ZF 4HP 20Damien Jorgensen100% (3)
- Aakriti 1Document92 pagesAakriti 1raghav bansalNo ratings yet
- Trade MarkDocument2 pagesTrade MarkRohit ThoratNo ratings yet
- 10 Killer Tips For Transcribing Jazz Solos - Jazz AdviceDocument21 pages10 Killer Tips For Transcribing Jazz Solos - Jazz Advicecdmb100% (2)