You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Severe and Multiple DisabilitiesDocument18 pagesSevere and Multiple DisabilitiesKavi Rehabian100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Spirit Releasement Protocol ListDocument4 pagesSpirit Releasement Protocol ListKristen Hammer100% (5)
- Diabetes EvaluationDocument3 pagesDiabetes Evaluatione-MedTools100% (3)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Important Question For Dialysis TechnicianDocument7 pagesImportant Question For Dialysis Technicianhunbaitmiki hinge100% (1)
- The Fitness Project 2018Document34 pagesThe Fitness Project 2018San joe50% (2)
- Peter Pan Syndrome Is A DeepDocument3 pagesPeter Pan Syndrome Is A DeeptucklertNo ratings yet
- Compilation of Nutri Ed ProgramsDocument5 pagesCompilation of Nutri Ed ProgramsDarwell Chann RosalesNo ratings yet
- Practice HPIDocument3 pagesPractice HPImedicalmatins100% (1)
- Therapeutic Modalities: Prepared By: John Patrick B. de JesusDocument22 pagesTherapeutic Modalities: Prepared By: John Patrick B. de JesusChiee A. CentinoNo ratings yet
- Test Bank For Counseling and Psychotherapy Theories in Context and Practice Skills Strategies and Techniques 3rd Edition John Sommers Flanagan Rita Sommers FlanaganDocument17 pagesTest Bank For Counseling and Psychotherapy Theories in Context and Practice Skills Strategies and Techniques 3rd Edition John Sommers Flanagan Rita Sommers Flanagancuthbertfinncx2nNo ratings yet
- Recurrent MeningitisDocument14 pagesRecurrent Meningitisidno1008No ratings yet
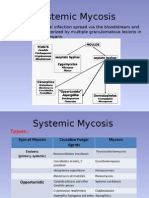
- MycosisDocument5 pagesMycosisMaiWahidGaberNo ratings yet
- Pathogenesis, Diagnosis and Treatment of Rasmussen EncephalitisDocument20 pagesPathogenesis, Diagnosis and Treatment of Rasmussen Encephalitisidno1008No ratings yet
- New Drugs For Epilepsy Mangement 1Document48 pagesNew Drugs For Epilepsy Mangement 1idno1008No ratings yet
- To Whom It May ConcernDocument1 pageTo Whom It May Concernidno1008No ratings yet
- Dr. ShahriarDocument1 pageDr. Shahriaridno1008No ratings yet
- EEG1Document13 pagesEEG1idno1008No ratings yet
- Musa IbrahimDocument3 pagesMusa Ibrahimidno1008No ratings yet
- Farzana ApuDocument1 pageFarzana Apuidno1008No ratings yet
- Admin Protocol AhdDocument1 pageAdmin Protocol Ahdidno1008No ratings yet
- Department of NeuromedicineDocument4 pagesDepartment of Neuromedicineidno1008No ratings yet
- Aseptic MeningitisDocument24 pagesAseptic Meningitisidno1008100% (1)
- Activities of Neuromedicine DepartmentDocument2 pagesActivities of Neuromedicine Departmentidno1008No ratings yet
- CIDPDocument21 pagesCIDPidno1008No ratings yet
- Daily StarDocument3 pagesDaily Staridno1008No ratings yet
- What To Do, When Gbs PT Fails To Respond To TreatmentDocument4 pagesWhat To Do, When Gbs PT Fails To Respond To Treatmentidno1008No ratings yet
- ParkinsonsDocument2 pagesParkinsonsidno1008No ratings yet
- Vestibular Rehabilitation ExercisesDocument1 pageVestibular Rehabilitation Exercisesidno1008No ratings yet
- StrokesDocument1 pageStrokesidno1008No ratings yet
- MigraneDocument1 pageMigraneidno1008No ratings yet
- Neck Exercises1Document3 pagesNeck Exercises1idno1008No ratings yet
- DementiaDocument1 pageDementiaidno1008No ratings yet
- Tugas Bahasa InggrisDocument14 pagesTugas Bahasa InggrisAlfin MT16No ratings yet
- CVC - B Braun - CertofixDocument14 pagesCVC - B Braun - CertofixMargaretta LimawanNo ratings yet
- Coagulation Profile in Diabetes MellitusDocument5 pagesCoagulation Profile in Diabetes MellitusAsfandyar RoghaniNo ratings yet
- Wastewater Disposal.Document266 pagesWastewater Disposal.FarazNo ratings yet
- By Sweta Kumari Summer Project-II Submitted ToDocument22 pagesBy Sweta Kumari Summer Project-II Submitted ToSudarshanKumar0% (1)
- The Tylenol Crisis: How Effective Public Relations Saved Johnson & JohnsonDocument11 pagesThe Tylenol Crisis: How Effective Public Relations Saved Johnson & JohnsonMuhamad LutfilahNo ratings yet
- Olympian Benchmark - 400mDocument15 pagesOlympian Benchmark - 400merwandumontNo ratings yet
- Case No 1:-Bio DataDocument8 pagesCase No 1:-Bio DataSarah Saqib Ahmad100% (1)
- Stroke Pathophysiology 1Document5 pagesStroke Pathophysiology 1Jeco ValdezNo ratings yet
- Congenital DiseaseDocument39 pagesCongenital DiseaseRavi SharmaNo ratings yet
- Status AsthmaticusDocument5 pagesStatus AsthmaticusHimmzNo ratings yet
- CTTDocument47 pagesCTTleizelgalvezNo ratings yet
- B PharmacyDocument26 pagesB PharmacyAkankshaNo ratings yet
- Reiki, Medicine & Self-Care With Pamela Miles: "Try Reiki" - Dr. Mehmet OzDocument10 pagesReiki, Medicine & Self-Care With Pamela Miles: "Try Reiki" - Dr. Mehmet OzSuresh NarenNo ratings yet
- Dream Abstracts PDFDocument61 pagesDream Abstracts PDFAlice Gina100% (1)
- LFS 233:module 5 Fats: College of Health Sciences Integrated Sciences DepartmentDocument65 pagesLFS 233:module 5 Fats: College of Health Sciences Integrated Sciences DepartmentHussain Ali100% (1)
- Lactose Intolerance: Diano, Gabriella Hilde Fanged, Paula Mandy Marrero, Xandra 9-KryptonDocument15 pagesLactose Intolerance: Diano, Gabriella Hilde Fanged, Paula Mandy Marrero, Xandra 9-KryptonArrianne AcopNo ratings yet
- A Comparative Study of Nutritional Status of Children Aged 11-14 Years of Low and High Economical Background, SuratDocument4 pagesA Comparative Study of Nutritional Status of Children Aged 11-14 Years of Low and High Economical Background, SuratEditor IJTSRDNo ratings yet
- Evaluation of The Health Beneficial Properties of The Aromatic Ether Myristicin, A Volatile Oil Derived From Various Plants SourcesDocument17 pagesEvaluation of The Health Beneficial Properties of The Aromatic Ether Myristicin, A Volatile Oil Derived From Various Plants SourcesIndra syahputraNo ratings yet