You might also like
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Carbide, Nitride and Boride Material Synthesis and ProcessingDocument674 pagesCarbide, Nitride and Boride Material Synthesis and ProcessingMarcia Gaby Cruz67% (3)
- Introduction To Non Destructive TestingDocument41 pagesIntroduction To Non Destructive Testingkmas161289% (9)
- Preview Chemistry IGCSEDocument76 pagesPreview Chemistry IGCSEAbdulrahman Mosfata0% (1)
- Complexometric TitrationDocument12 pagesComplexometric TitrationBwhzad HameedNo ratings yet
- MTPCL - WTP O&m ManualDocument62 pagesMTPCL - WTP O&m Manualm_ganesh1983100% (4)
- Tugas PPM Deny Saputro Arifin 113170039Document9 pagesTugas PPM Deny Saputro Arifin 113170039Vira IrnandaNo ratings yet
- Food Fish Processing NotesDocument14 pagesFood Fish Processing NotesRoselyn MyerNo ratings yet
- 10 Main Personal Protective EquipmentDocument7 pages10 Main Personal Protective EquipmentDaniel CastilloNo ratings yet
- For The Determination of Precious Metals in Autocatalyst SamplesDocument6 pagesFor The Determination of Precious Metals in Autocatalyst SamplesScumpika ElenaNo ratings yet
- Infrared Optical Materials and Their Antireflection CoatingsDocument5 pagesInfrared Optical Materials and Their Antireflection CoatingsnguyenthanhhopNo ratings yet
- Kuala Lumpur Kepong Berhad - WikipediaDocument17 pagesKuala Lumpur Kepong Berhad - Wikipedianoel.manroeNo ratings yet
- Vocabular PDFDocument5 pagesVocabular PDFAndra Ch123No ratings yet
- PNS 113 Rebars PDFDocument12 pagesPNS 113 Rebars PDFKenneth PenianoNo ratings yet
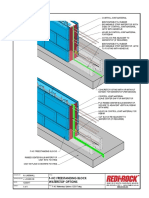
- F-HC Waterstop Options 122017Document1 pageF-HC Waterstop Options 122017ED WARMONDNo ratings yet
- Pozzolith 80 PDFDocument2 pagesPozzolith 80 PDFDoby YuniardiNo ratings yet
- Mixing A Balanced Nutrient SolutionDocument16 pagesMixing A Balanced Nutrient SolutionRómulo Del ValleNo ratings yet
- Biodegradable Polymers For Sustainable Packaging Applications - A ReviewDocument12 pagesBiodegradable Polymers For Sustainable Packaging Applications - A ReviewAngelito AraxielNo ratings yet
- Talaat A.Kader: Country ManagerDocument6 pagesTalaat A.Kader: Country ManagermohammedNo ratings yet
- AOAC Official Method - 962 - 16 - Sulfurous Acid (Total) in Food - Modifie...Document2 pagesAOAC Official Method - 962 - 16 - Sulfurous Acid (Total) in Food - Modifie...mustafa kaya100% (1)
- ادوية التخدير 2Document2 pagesادوية التخدير 2b2ddfnvfp6No ratings yet
- ACG Associated Capsules PVT LTD: A Member of ACG WorldwideDocument4 pagesACG Associated Capsules PVT LTD: A Member of ACG Worldwidepeter mackey mamani mamanchura100% (1)
- Project On Powder Dispensing System of Sand 3d PrintingDocument101 pagesProject On Powder Dispensing System of Sand 3d PrintingSameer MandaogadeNo ratings yet
- Preparation and Evaluation of Controlled Release Tablets Containing Mefenamic Acid 2161 1459.1000107Document3 pagesPreparation and Evaluation of Controlled Release Tablets Containing Mefenamic Acid 2161 1459.1000107Rike YulianingtyasNo ratings yet
- Pharmacology AlgesiologyDocument4 pagesPharmacology AlgesiologyCpopNo ratings yet
- Kinetics of The Selective Hydrogenation of Phenol To Cyclohexanone Over A Pd-Alumina CatalystDocument8 pagesKinetics of The Selective Hydrogenation of Phenol To Cyclohexanone Over A Pd-Alumina CatalystTaylor PennaNo ratings yet
- Class 12 Chemistry Biomolecules PyqDocument11 pagesClass 12 Chemistry Biomolecules PyqRakesh AgarwalNo ratings yet
- C898C898M 09.pdf (EngPedia - Ir)Document14 pagesC898C898M 09.pdf (EngPedia - Ir)Hossein DoudiNo ratings yet
- Astm A479Document7 pagesAstm A479Martin RomeroNo ratings yet
- Effects of Fly Ash and Silica Fume On The Resistance of Mortar To Sulfuric Acid and Sulfate AttackDocument10 pagesEffects of Fly Ash and Silica Fume On The Resistance of Mortar To Sulfuric Acid and Sulfate AttackMaziar Mehravar100% (1)
- Retrofitting of BuildingDocument5 pagesRetrofitting of BuildingEmily UyNo ratings yet