You might also like
- Best Trusts and Estates OutlineDocument84 pagesBest Trusts and Estates OutlineJavi Luis100% (4)
- Positioning ChecklistDocument2 pagesPositioning ChecklistMark Terence Padua AbrenicaNo ratings yet
- KISS Notes The World CommunicatesDocument30 pagesKISS Notes The World CommunicatesJenniferBackhus100% (4)
- 10 Tips For Better Legal WritingDocument12 pages10 Tips For Better Legal WritingYvzNo ratings yet
- Survey of World HistoryDocument77 pagesSurvey of World Historyrufinus ondiekiNo ratings yet
- Absolute Community of Property vs. Conjugal Partnership of GainsDocument7 pagesAbsolute Community of Property vs. Conjugal Partnership of GainsJill LeaNo ratings yet
- Abruptio Placentae Case StudyDocument4 pagesAbruptio Placentae Case StudyMonchee YusonNo ratings yet
- Abruptio Placenta: Prepared By: Claire Alvarez Ongchua, RNDocument42 pagesAbruptio Placenta: Prepared By: Claire Alvarez Ongchua, RNclaireaongchua1275100% (2)
- Incompetent CervixDocument29 pagesIncompetent CervixCyrelle Jen TorresNo ratings yet
- RH Incompatibility: DR - Minal M. Patil Dr. Jyotsna P. PatilDocument27 pagesRH Incompatibility: DR - Minal M. Patil Dr. Jyotsna P. Patilchitushri100% (1)
- 5 - Abortion or MiscarriageDocument43 pages5 - Abortion or Miscarriageasifdawar2011No ratings yet
- RH IncompatibilityDocument7 pagesRH IncompatibilityMichael CabiliNo ratings yet
- Incompetent CervixDocument4 pagesIncompetent CervixCharm Arroyo100% (1)
- RH IncompatibilityDocument9 pagesRH IncompatibilityJohn BardeenNo ratings yet
- RH Incompatibility: Go ToDocument4 pagesRH Incompatibility: Go ToFadhila AnasNo ratings yet
- Case Presentation: Placenta Previa: Crissa Marie D. PinedaDocument42 pagesCase Presentation: Placenta Previa: Crissa Marie D. PinedaCrissa PinedaNo ratings yet
- Neonatal Case Presentation 1Document5 pagesNeonatal Case Presentation 1Rexelle RamosNo ratings yet
- Pregnancy Induced Hypertension (Pih)Document56 pagesPregnancy Induced Hypertension (Pih)shandi23100% (5)
- Small For Gestational Age InfantsDocument3 pagesSmall For Gestational Age InfantsKhemz Dalde Lim100% (1)
- Premature Rupture of MembranesDocument4 pagesPremature Rupture of MembranesNikko Pabico67% (3)
- Uterine AtonyDocument3 pagesUterine AtonyArsheina Paradji100% (1)
- Small For Gestational AgeDocument14 pagesSmall For Gestational AgeMaria Delia Salvado100% (2)
- Abruptio Placenta FullDocument10 pagesAbruptio Placenta FullChester ManaloNo ratings yet
- Premature Rupture of MembranesDocument33 pagesPremature Rupture of MembranesSarang Lee100% (1)
- PromDocument33 pagesPromkisNo ratings yet
- Abruptio PlacentaDocument13 pagesAbruptio Placentamiss RN92% (12)
- What Is RH IncompatibilityDocument22 pagesWhat Is RH IncompatibilityKimsha ConcepcionNo ratings yet
- ABO IncompatibilityDocument9 pagesABO IncompatibilityJuli-anne Villarico AndresNo ratings yet
- Periods of Nursing HistoryDocument38 pagesPeriods of Nursing HistoryJeny Pearl Hijosa0% (1)
- Placenta Praevia and Placenta AccretaDocument75 pagesPlacenta Praevia and Placenta AccretaNurul Fahmiza TumiranNo ratings yet
- Neonatal Hyperbilirubinemia and JaundiceDocument8 pagesNeonatal Hyperbilirubinemia and JaundiceAndreea GeorgianaNo ratings yet
- RH Incompatibility - RupeshDocument4 pagesRH Incompatibility - Rupeshrupesh_mamidi100% (2)
- Uterine RuptureDocument19 pagesUterine RuptureAna Denise Quinajon0% (1)
- Meconium Aspiration Syndrome (MAS)Document12 pagesMeconium Aspiration Syndrome (MAS)Angela AmaoNo ratings yet
- RH Incompatibil TY: What Is RH Incompatibility?Document15 pagesRH Incompatibil TY: What Is RH Incompatibility?Jannah Marie A. DimaporoNo ratings yet
- RH IncompatibilityDocument10 pagesRH IncompatibilityVernie Dinglasa GeligNo ratings yet
- RH IncompatibilityDocument3 pagesRH IncompatibilityMima Fatimah LuthfieNo ratings yet
- 158 Carino vs. CADocument2 pages158 Carino vs. CAFrancesca Isabel Montenegro67% (3)
- OligohydramniosDocument4 pagesOligohydramniossalamredNo ratings yet
- ABO Incompatibility: By: Marvi Mae Jimena Rosean Marvi Joy M. YunsayDocument14 pagesABO Incompatibility: By: Marvi Mae Jimena Rosean Marvi Joy M. Yunsaysagameteiro100% (1)
- Fetal DistressDocument4 pagesFetal DistressAmira Attya100% (7)
- Complications During Labor and Delivery - HardDocument19 pagesComplications During Labor and Delivery - Hardkrizele ann santosNo ratings yet
- Hydatidiform Mole AnahistoDocument11 pagesHydatidiform Mole AnahistoIanMayNo ratings yet
- Incompetent CervixDocument5 pagesIncompetent CervixNaidin Catherine De Guzman-Alcala100% (1)
- Role of Communication in BusinessDocument3 pagesRole of Communication in Businessmadhu motkur100% (2)
- RH IncompatibilityDocument9 pagesRH IncompatibilitySerafin Dimalaluan III50% (2)
- RH Disease and ABO IncompatibilityDocument21 pagesRH Disease and ABO Incompatibilityjeezislove617No ratings yet
- Management Placenta PreviaDocument24 pagesManagement Placenta PreviaMuhammad RifaldiNo ratings yet
- Φ PathophysiologyDocument4 pagesΦ PathophysiologyMariah AshooriyanNo ratings yet
- RH IncompatibilityDocument35 pagesRH Incompatibilityaparna100% (1)
- CPD, Dystocia, Fetal Distress OutputDocument8 pagesCPD, Dystocia, Fetal Distress OutputJohn Dave AbranNo ratings yet
- HyperbilirubinemiaDocument10 pagesHyperbilirubinemiachiboogs456100% (1)
- DystociaDocument31 pagesDystociamarsan120% (1)
- Cervical IncompetenceDocument3 pagesCervical IncompetencekarlacamilledeleonNo ratings yet
- Ectopic Pregnancy - CSDocument14 pagesEctopic Pregnancy - CSMASII100% (1)
- Idiophatic Thrombocytopenic Purpura (ITP) in PregnancyDocument27 pagesIdiophatic Thrombocytopenic Purpura (ITP) in PregnancyAdietya Bima PrakasaNo ratings yet
- Ophthalmia NeonatorumDocument19 pagesOphthalmia NeonatorumSanthu Tvm100% (1)
- Fetal Distress Case DiscussionDocument55 pagesFetal Distress Case DiscussionHafsah G.No ratings yet
- Presentation ABO & RH IncompactDocument33 pagesPresentation ABO & RH IncompactPinanong PimsuwanNo ratings yet
- Gestational Diabetes Mellitus (GDM)Document24 pagesGestational Diabetes Mellitus (GDM)asyrafali93No ratings yet
- Pathophysiology of Erythroblastosis Fetalis - RH IsoimmunizationDocument1 pagePathophysiology of Erythroblastosis Fetalis - RH IsoimmunizationRalph Delos SantosNo ratings yet
- Neonatal HyperbilirubinemiaDocument36 pagesNeonatal HyperbilirubinemiamahmmoudeltaweelNo ratings yet
- Postpartum HemorrhageDocument3 pagesPostpartum HemorrhageClaire Canapi BattadNo ratings yet
- PROM Care PlanDocument2 pagesPROM Care PlanMariagmzNo ratings yet
- Pathophysiology of Hypersensitivity Type IIDocument2 pagesPathophysiology of Hypersensitivity Type IItwin_smartyNo ratings yet
- RH IncompatibilityDocument6 pagesRH IncompatibilityEly TaNo ratings yet
- Background: RH IncompatibilityDocument8 pagesBackground: RH IncompatibilityBrett StevensonNo ratings yet
- Rhalloimmunization 180317110948Document57 pagesRhalloimmunization 180317110948BIRHANE TESFAYNo ratings yet
- RH IncompatibilityDocument4 pagesRH IncompatibilityMADULI, Marlone G.No ratings yet
- Breastfeeding Without Birthing 3Document6 pagesBreastfeeding Without Birthing 3Mark Terence Padua AbrenicaNo ratings yet
- 4 Short Stories That Will Change The Way You Think: WR I Tten by M Arc C He Rnoff // 84 Comme NtsDocument6 pages4 Short Stories That Will Change The Way You Think: WR I Tten by M Arc C He Rnoff // 84 Comme NtsMark Terence Padua AbrenicaNo ratings yet
- Battle Realms Editor CompiledDocument32 pagesBattle Realms Editor CompiledMark Terence Padua AbrenicaNo ratings yet
- Schema and Reading Comprehension Relative To Academic Performance of Grade 10 Students at Binulasan Integrated SchoolDocument12 pagesSchema and Reading Comprehension Relative To Academic Performance of Grade 10 Students at Binulasan Integrated SchoolShenly EchemaneNo ratings yet
- Types of Editorial Texts: Queen Zayra Dela Rosa Francisco DagohoyDocument8 pagesTypes of Editorial Texts: Queen Zayra Dela Rosa Francisco DagohoyAkiro KaitoNo ratings yet
- Ashwin Murthy TortsDocument28 pagesAshwin Murthy Tortssaurabh kapurNo ratings yet
- Agatthiyar's Saumya Sagaram - A Quick Summary of The Ashta KarmaDocument5 pagesAgatthiyar's Saumya Sagaram - A Quick Summary of The Ashta KarmaBujji JohnNo ratings yet
- RB September 2014 The One Thing Kekuatan Fokus Untuk Mendorong ProduktivitasDocument2 pagesRB September 2014 The One Thing Kekuatan Fokus Untuk Mendorong ProduktivitasRifat TaopikNo ratings yet
- Assessing Implicit Motives With An Online VersionDocument16 pagesAssessing Implicit Motives With An Online VersionWunderkindNo ratings yet
- Dacera Vs Dela SernaDocument2 pagesDacera Vs Dela SernaDarlo HernandezNo ratings yet
- Compiler Design MCQ Question Bank Last Update 29-Dec-20202 Page 1 of 18Document18 pagesCompiler Design MCQ Question Bank Last Update 29-Dec-20202 Page 1 of 18SOMENATH ROY CHOUDHURYNo ratings yet
- Week 1 Reading 2Document35 pagesWeek 1 Reading 2Prakhar ManasNo ratings yet
- Dharnish ReportDocument13 pagesDharnish Reportdarshan75% (4)
- The SacrificeDocument3 pagesThe SacrificeRoseann Hidalgo ZimaraNo ratings yet
- Different Types of Merging Using Data Step or Proc SQL in SASDocument3 pagesDifferent Types of Merging Using Data Step or Proc SQL in SAShimaNo ratings yet
- Battleship PotemkinDocument7 pagesBattleship PotemkinMariusOdobașa100% (1)
- Engineering Code of EthicsDocument4 pagesEngineering Code of EthicsBeth Beth DiancoNo ratings yet
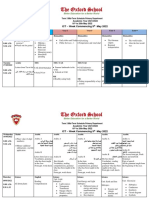
- Term 3 Mid-Term Assessment ScheduleDocument9 pagesTerm 3 Mid-Term Assessment ScheduleRabia MoeedNo ratings yet
- Help Us Clean The Government HospitalsDocument3 pagesHelp Us Clean The Government HospitalsSelva GanapathyNo ratings yet
- Knowledge Versus OpinionDocument20 pagesKnowledge Versus OpinionShumaila HameedNo ratings yet
- Kutuzov A Life in War and Peace Alexander Mikaberidze 2 Full ChapterDocument67 pagesKutuzov A Life in War and Peace Alexander Mikaberidze 2 Full Chapterjanice.brooks978100% (6)
- Sampling TechDocument5 pagesSampling TechJAMZ VIBESNo ratings yet
- DPC Rough Draft by Priti Guide (1953)Document6 pagesDPC Rough Draft by Priti Guide (1953)Preeti GuideNo ratings yet
- MBA ABM SyllabusDocument33 pagesMBA ABM Syllabuszinga007No ratings yet
- IBbusiness Revision NotesDocument58 pagesIBbusiness Revision NotesMayankJhaNo ratings yet