You might also like
- PSAP 2019 Dyslipidemia PDFDocument24 pagesPSAP 2019 Dyslipidemia PDFdellykets_323822919No ratings yet
- Anaesthetic Drug Crib Sheet-8 PDFDocument1 pageAnaesthetic Drug Crib Sheet-8 PDFSlaviša Kovačević100% (1)
- PSAP 2019 Dyslipidemia PDFDocument24 pagesPSAP 2019 Dyslipidemia PDFdellykets_323822919No ratings yet
- Slide Himawan Liphantyl Febr 2021Document43 pagesSlide Himawan Liphantyl Febr 2021Muliani AwalNo ratings yet
- (Pertemuan 6) Pharmacotherapy of Hypertension - 2022 - RevisiDocument47 pages(Pertemuan 6) Pharmacotherapy of Hypertension - 2022 - RevisiREFITHA PUTRINo ratings yet
- PAD Medical TreatmentDocument17 pagesPAD Medical Treatmentmeliser86No ratings yet
- Cholesterol-Lowering Agents Statins-For Everyone? 2019Document10 pagesCholesterol-Lowering Agents Statins-For Everyone? 2019Luis Alberto Alvarez AnkassNo ratings yet
- The Importance of Potential Statin in High Risk PatientDocument56 pagesThe Importance of Potential Statin in High Risk PatientAidil Fittriani AyuNo ratings yet
- Evidence Based PADDocument13 pagesEvidence Based PADIrma SihotangNo ratings yet
- COMPASS by RISK STRATDocument10 pagesCOMPASS by RISK STRATMiguel GonzalezNo ratings yet
- Atherothrombosis Drugs Compendium: Cholesterol-Lowering AgentsDocument17 pagesAtherothrombosis Drugs Compendium: Cholesterol-Lowering AgentsSri MaryatiNo ratings yet
- Dyslipidemia & Residual RiskDocument26 pagesDyslipidemia & Residual RiskDan LeeNo ratings yet
- ArtovastatinDocument3 pagesArtovastatinSL Hanna NebridaNo ratings yet
- VHRM 23468 Indications For and Utilization of Angiotensin At1 Receptor 092311Document18 pagesVHRM 23468 Indications For and Utilization of Angiotensin At1 Receptor 092311Arbi SulaimanNo ratings yet
- Reviews: Statins in The Primary Prevention of Cardiovascular DiseaseDocument12 pagesReviews: Statins in The Primary Prevention of Cardiovascular DiseaseCrischentian BrinzaNo ratings yet
- Aspirin and Low Dose Rivaroxaban - The Dual Pathway Concept in Patients With Stable Atherosclerotic Disease: A Comprehensive ReviewDocument24 pagesAspirin and Low Dose Rivaroxaban - The Dual Pathway Concept in Patients With Stable Atherosclerotic Disease: A Comprehensive ReviewWilliam ChokNo ratings yet
- Heartjnl 2019 316164.fullDocument9 pagesHeartjnl 2019 316164.fulltemesgenNo ratings yet
- Lower Extremity Arterial Disease: Medical Management and Decision MakingDocument26 pagesLower Extremity Arterial Disease: Medical Management and Decision MakingGhany Hendra WijayaNo ratings yet
- The Different Therapeutic Choices With Arbs. Which One To Give? When? Why?Document12 pagesThe Different Therapeutic Choices With Arbs. Which One To Give? When? Why?Jonathan Ian ArinsolNo ratings yet
- Approaches To Peripheral Artery Disease in DiabetesDocument18 pagesApproaches To Peripheral Artery Disease in DiabetesNabita AuliaNo ratings yet
- 01 Cir 0000038923 61628 3DDocument3 pages01 Cir 0000038923 61628 3DGet BetterNo ratings yet
- 2019 EVC LacunarDocument24 pages2019 EVC LacunarJuan Pablo B. FloresNo ratings yet
- Efek Statin Dalam Menurunkan Angka Kejadian Penyakit KardiovaskularDocument6 pagesEfek Statin Dalam Menurunkan Angka Kejadian Penyakit KardiovaskularAndrie WigunaNo ratings yet
- Drugs Mechanism of Action Indication Contraindication Adverse EffectsDocument2 pagesDrugs Mechanism of Action Indication Contraindication Adverse Effectsisprikitik3No ratings yet
- Statins and Beyond Concurrent Strategies For Prevention of Cardiovascular Disease in Patients WiDocument17 pagesStatins and Beyond Concurrent Strategies For Prevention of Cardiovascular Disease in Patients WiMamad TrihatmowidjoyoNo ratings yet
- The Role of Statins in The Prevention of PreeclampDocument11 pagesThe Role of Statins in The Prevention of PreeclampEcaterina Sorto de ArgeñalNo ratings yet
- Combination Lipid-Lowering Therapy As First-LineDocument4 pagesCombination Lipid-Lowering Therapy As First-LinejoNo ratings yet
- A Comprehensive Review On Antithrombotic Therapy For Peripheral Artery DiseaseDocument8 pagesA Comprehensive Review On Antithrombotic Therapy For Peripheral Artery DiseasesunhaolanNo ratings yet
- Kelompok 1Document14 pagesKelompok 1Aurent WidjanarkoNo ratings yet
- Diabetic Retinopathy Screening Update: Epidemiology Pathophysiology and ClassificationDocument6 pagesDiabetic Retinopathy Screening Update: Epidemiology Pathophysiology and ClassificationAulia Eka PurwaniNo ratings yet
- Art EVC IsquémicoDocument22 pagesArt EVC IsquémicoarrlyNo ratings yet
- Pulmonary EmbolismDocument17 pagesPulmonary EmbolismSNo ratings yet
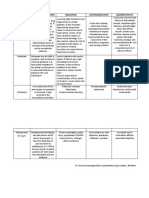
- College of Nursing and Midwifery: Mabini Colleges Daet, Camarines NorteDocument10 pagesCollege of Nursing and Midwifery: Mabini Colleges Daet, Camarines NorteMa. Sheenadel ZamudioNo ratings yet
- The Different Therapeutic Choices With Arbs. Which One To Give? When? Why?Document28 pagesThe Different Therapeutic Choices With Arbs. Which One To Give? When? Why?Rajeev GuptaNo ratings yet
- Ca UtiDocument14 pagesCa UtiBayu TrigunaNo ratings yet
- An Opinion: Chelation Therapy of AtherosclerosisDocument4 pagesAn Opinion: Chelation Therapy of Atherosclerosissinta dwi andariNo ratings yet
- Management of Hypertension in DMDocument22 pagesManagement of Hypertension in DMNathania Nadia BudimanNo ratings yet
- Preventing Cardiovascular Disease in Patients With.2 PDFDocument3 pagesPreventing Cardiovascular Disease in Patients With.2 PDFbacharelado2010No ratings yet
- Summary - Cardio-Oncology-2016-for Web PDFDocument2 pagesSummary - Cardio-Oncology-2016-for Web PDFDya AndryanNo ratings yet
- Jurnal InternaDocument11 pagesJurnal InternaRamlah AndariasNo ratings yet
- Diabetes For Cardiologists Practical Issues in Diagnosis and ManagementDocument12 pagesDiabetes For Cardiologists Practical Issues in Diagnosis and ManagementLuis Alberto OrtizNo ratings yet
- Lee Et Al 2023 Combination Lipid Lowering Therapy in Patients Undergoing Percutaneous Coronary InterventionDocument10 pagesLee Et Al 2023 Combination Lipid Lowering Therapy in Patients Undergoing Percutaneous Coronary InterventionKardiologi ManadoNo ratings yet
- PENAFIEL M5 April2-2023Document11 pagesPENAFIEL M5 April2-2023Precious Valerie PenafielNo ratings yet
- Safety and Efficacy of Statin TherapyDocument13 pagesSafety and Efficacy of Statin TherapyAlexa ArceNo ratings yet
- SOLU-MEDROL Sterile Powder IsDocument3 pagesSOLU-MEDROL Sterile Powder IsMARIAM A JAJINo ratings yet
- Jaha 116 004909 PDFDocument8 pagesJaha 116 004909 PDFLisbeth MarbunNo ratings yet
- Varma - Cardio Oncology SM121917Document12 pagesVarma - Cardio Oncology SM121917Gabriela Araya MedranoNo ratings yet
- Contemporary PAD ManagementDocument27 pagesContemporary PAD ManagementMaria PopNo ratings yet
- Name of Drug Content Class and Mechanism of Action (MOA) Indication/s Contraindication/s Side Effects (Pere System) Nursing ConsiderationsDocument8 pagesName of Drug Content Class and Mechanism of Action (MOA) Indication/s Contraindication/s Side Effects (Pere System) Nursing ConsiderationsJustin John NavarroNo ratings yet
- Use of Statins and The Incidence of Type 2 Diabetes MellitusDocument6 pagesUse of Statins and The Incidence of Type 2 Diabetes MellitusBenji MincholaNo ratings yet
- Sodium Retention in Heart Failure and CirrhosisDocument7 pagesSodium Retention in Heart Failure and Cirrhosisnu idNo ratings yet
- Circulationaha 116 023164Document16 pagesCirculationaha 116 023164Wisnu AdryantoNo ratings yet
- Revision Lipidos2Document15 pagesRevision Lipidos2andres herreraNo ratings yet
- Role of Bempedoic Acid in Dyslipidemia ManagementDocument13 pagesRole of Bempedoic Acid in Dyslipidemia ManagementkkkljlkjNo ratings yet
- Combination Antiplatelet and Oral Anticoagulant Therapy in Patients With Coronary and Peripheral Artery Disease 2018Document16 pagesCombination Antiplatelet and Oral Anticoagulant Therapy in Patients With Coronary and Peripheral Artery Disease 2018DrHellenNo ratings yet
- Chemotherapy-Induced DysfunctionDocument13 pagesChemotherapy-Induced DysfunctionZulkarnain MuinNo ratings yet
- CRUSADE ScoreDocument10 pagesCRUSADE ScoreYulian 53No ratings yet
- Circresaha 117 311586Document15 pagesCircresaha 117 311586jimNo ratings yet
- Applicability of Recent Dyslipidemia Guidelines in Clinical PracticeDocument4 pagesApplicability of Recent Dyslipidemia Guidelines in Clinical PracticeDokter FebyanNo ratings yet
- What Does COMPASS AddDocument8 pagesWhat Does COMPASS AddMiguel GonzalezNo ratings yet
- Compendium on Cardiomyopathies - Basics, Therapeutics, and PerspectivesFrom EverandCompendium on Cardiomyopathies - Basics, Therapeutics, and PerspectivesNo ratings yet
- Exams 3rd Sec الجمهوريهDocument2 pagesExams 3rd Sec الجمهوريهactive learning educationNo ratings yet
- Practica Dermofarmacia Semana 14Document6 pagesPractica Dermofarmacia Semana 14Diego ANo ratings yet
- Composition and Quality of Lentil Medik) : A Review: (Lens CulinarisDocument17 pagesComposition and Quality of Lentil Medik) : A Review: (Lens CulinarisKarla MontesNo ratings yet
- Certificate of Analysis Arctic CLO Strawberry 16oz - 161973 PDFDocument1 pageCertificate of Analysis Arctic CLO Strawberry 16oz - 161973 PDFjayjonbeachNo ratings yet
- Kitar KrebsDocument5 pagesKitar KrebsAlfonso RobertNo ratings yet
- GlycosylationDocument9 pagesGlycosylationĐỗ Thanh TùngNo ratings yet
- Dr. Suryono, SPJPDocument26 pagesDr. Suryono, SPJPPowool LalaNo ratings yet
- ROSADocument9 pagesROSAREZA ARY FACHRURROZINo ratings yet
- Camfil Air Filter - Carbon, G3, G4Document4 pagesCamfil Air Filter - Carbon, G3, G4Quang Dong100% (1)
- Total Synthesis of NorzoanthamineDocument7 pagesTotal Synthesis of NorzoanthamineAyush BoseNo ratings yet
- Product Range PharmaDocument2 pagesProduct Range PharmaNadie NingunoNo ratings yet
- '' SQ-FFQ PPGDocument165 pages'' SQ-FFQ PPGRaudhatul AgustiaNo ratings yet
- 8 - Secondary Metabolites - TERPENOIDS ALKALOIDS PHENOLICS PDFDocument82 pages8 - Secondary Metabolites - TERPENOIDS ALKALOIDS PHENOLICS PDFFCiênciasNo ratings yet
- Carbohydrates Post LabDocument4 pagesCarbohydrates Post LabAki OtaniNo ratings yet
- GlycosidesDocument2 pagesGlycosidesNishamolKSNo ratings yet
- Marking of Polymeric Parts: Nissan Engineering StandardDocument14 pagesMarking of Polymeric Parts: Nissan Engineering StandardKarthic BhrabuNo ratings yet
- Valsartan Products NOT Recalled 120042108Document14 pagesValsartan Products NOT Recalled 120042108smorrison06No ratings yet
- 1.5 LipidsDocument19 pages1.5 Lipidsasifh76543No ratings yet
- Grading Rubric For DNA ModelDocument2 pagesGrading Rubric For DNA ModelDebbie Ann LaguindabNo ratings yet
- Daftar Permintaan Pustu-2Document15 pagesDaftar Permintaan Pustu-2Yanti FitryNo ratings yet
- Oxidative Stress Free Radicals Flipped Class - 2021 - 02 (1) 2Document18 pagesOxidative Stress Free Radicals Flipped Class - 2021 - 02 (1) 2Diran TerzyanNo ratings yet
- TOLLENSDocument5 pagesTOLLENSDDS (Dingdong Dantes Supporter)No ratings yet
- List Obat Beserta Kelas TerapinyaDocument4 pagesList Obat Beserta Kelas TerapinyaSellymarlinaleeNo ratings yet
- Reduction Agents Organic ChemistryDocument55 pagesReduction Agents Organic ChemistryvgvijuNo ratings yet
- Pemakaian Obat RasionalDocument62 pagesPemakaian Obat RasionalMARTININo ratings yet
- ZdecDocument10 pagesZdecgbiyer1234No ratings yet
- 18章 PDFDocument41 pages18章 PDF台師大蔡銘揚No ratings yet
- Zenotis Healthcare Hospital List Wef 01 Aug 2022 - All Divisions UpdatedDocument20 pagesZenotis Healthcare Hospital List Wef 01 Aug 2022 - All Divisions UpdatedMANDEEP KUMARNo ratings yet