You might also like
- Prior Authorization Request FormDocument3 pagesPrior Authorization Request FormvanessaNo ratings yet
- JIT 2363 Authorization To Release Med RecordsDocument2 pagesJIT 2363 Authorization To Release Med Recordsalan benedettaNo ratings yet
- Format Pre EmploymentDocument10 pagesFormat Pre EmploymentNurman HidayatNo ratings yet
- Adolescent ResilienceDocument53 pagesAdolescent ResilienceJoan Vianney Clare JudayaNo ratings yet
- Susan Kun Leddy-Integrative Health Promotion - Conceptual Bases For Nursing Practice, Second Edition (2005) PDFDocument508 pagesSusan Kun Leddy-Integrative Health Promotion - Conceptual Bases For Nursing Practice, Second Edition (2005) PDFDiah Hastuti100% (2)
- Guide To The Sarbanes-Oxley Act: IT Risks and Controls: Second EditionDocument45 pagesGuide To The Sarbanes-Oxley Act: IT Risks and Controls: Second EditiongamallofNo ratings yet
- Corporate Hse AuditDocument21 pagesCorporate Hse AuditKukuh Widodo100% (3)
- HIM 200 Health RecordDocument32 pagesHIM 200 Health RecordMaryamNo ratings yet
- Medical Certificate 2Document2 pagesMedical Certificate 2Aditeya Shukla100% (1)
- Chapter 1 and 2 (LATEST)Document34 pagesChapter 1 and 2 (LATEST)Jade MonteverosNo ratings yet
- Laboratory and Workshop HandbookDocument134 pagesLaboratory and Workshop HandbookBidhan RajkarnikarNo ratings yet
- Participant Registration FORMSDocument6 pagesParticipant Registration FORMSbernardhhi100% (1)
- 2034 PDFDocument2 pages2034 PDFJagyanseni BeheraNo ratings yet
- QR-RCP-009 Authorization For Disclosure of Health InformationRecords - Rev07Document1 pageQR-RCP-009 Authorization For Disclosure of Health InformationRecords - Rev07Yel BNo ratings yet
- Telepsychiatry Consent Form PSPCDocument2 pagesTelepsychiatry Consent Form PSPCTimothy NguyenNo ratings yet
- Authorization For Release of Medical InformationDocument1 pageAuthorization For Release of Medical Informationcig3fNo ratings yet
- Attending Physicians Statement Crisis Cover Renal Failure - 041222Document2 pagesAttending Physicians Statement Crisis Cover Renal Failure - 041222max leeNo ratings yet
- Briettavasser Job 33 Form 3Document1 pageBriettavasser Job 33 Form 3api-669728207No ratings yet
- Special BenefitDocument20 pagesSpecial BenefitHihiNo ratings yet
- AppForm - GroupMedIns - Member - 2016-06 (June14)Document3 pagesAppForm - GroupMedIns - Member - 2016-06 (June14)Ruchie EtolleNo ratings yet
- Medical Release FormDocument1 pageMedical Release Formmr_b123No ratings yet
- Medical Examintation Report: Document No MTIPL/HR/F0006 1Document1 pageMedical Examintation Report: Document No MTIPL/HR/F0006 1Kabir ShelkeNo ratings yet
- ConsentDocument2 pagesConsentNobel LaureateNo ratings yet
- Consent For Minor Dental PDFDocument2 pagesConsent For Minor Dental PDFJanNo ratings yet
- AXA Hypertension QuestionnaireDocument2 pagesAXA Hypertension QuestionnaireClaudine Limasa TabudlongNo ratings yet
- HOH Volunteer FormsDocument4 pagesHOH Volunteer FormsbernardhhiNo ratings yet
- Attending Physicians Statement Crisis Cover Muscular Dystrophy - 041222Document2 pagesAttending Physicians Statement Crisis Cover Muscular Dystrophy - 041222laraNo ratings yet
- Release MedicalInfo TODocument1 pageRelease MedicalInfo TOChristinah Tamby LewanikaNo ratings yet
- Attending Physicians Statement Crisis Cover Major Organ Transplant - 041222Document2 pagesAttending Physicians Statement Crisis Cover Major Organ Transplant - 041222max leeNo ratings yet
- Medicare Insurance Claim Form: PolicyholderDocument2 pagesMedicare Insurance Claim Form: PolicyholdertagashiiNo ratings yet
- Pre Employment Medical Declaration Form - 2022Document2 pagesPre Employment Medical Declaration Form - 2022Neel GhoshNo ratings yet
- Physician'S Statement For Medical Review Unit: Please Print or TypeDocument2 pagesPhysician'S Statement For Medical Review Unit: Please Print or TypeCristian De la cruz cantilloNo ratings yet
- MFC PDFDocument5 pagesMFC PDFdipmipNo ratings yet
- Med ReleaseDocument1 pageMed ReleaseMatt SolheimNo ratings yet
- 00000Document2 pages00000Jake CopradeNo ratings yet
- Medical CertificateDocument2 pagesMedical CertificatelekacaNo ratings yet
- Clal Health Insurance Company LTD.: Healthy & SureDocument4 pagesClal Health Insurance Company LTD.: Healthy & SureM.I. BdaNo ratings yet
- Claim FormDocument1 pageClaim FormBunga Sephtiana IINo ratings yet
- Patient Registration Form: How Did You Hear About Bay Area Eye Institute?Document11 pagesPatient Registration Form: How Did You Hear About Bay Area Eye Institute?leivis cabreraNo ratings yet
- REV - Outpatient Claim Form - AIADocument2 pagesREV - Outpatient Claim Form - AIAYen SylvaniNo ratings yet
- Courtney Broton Job33-Form3Document1 pageCourtney Broton Job33-Form3api-550569140No ratings yet
- Member Addition FormDocument3 pagesMember Addition FormharshitakoutaNo ratings yet
- Claims Aps Hi MR SurgicalDocument3 pagesClaims Aps Hi MR SurgicalRudolf CunananNo ratings yet
- So Physical Form HighlightedDocument2 pagesSo Physical Form Highlightedapi-267917820No ratings yet
- Adult Full Assessment With MSEDocument7 pagesAdult Full Assessment With MSEmary grace bialenNo ratings yet
- Claim FormDocument1 pageClaim FormFAZILNo ratings yet
- Allina Health Authorization To Release and Disclose Patient InformationDocument2 pagesAllina Health Authorization To Release and Disclose Patient InformationSonof Godd0% (1)
- New Axa FormDocument2 pagesNew Axa FormAzrul Azuar Azrul Azuar100% (1)
- Suspected Adverse Drug ReactionsDocument2 pagesSuspected Adverse Drug ReactionsBBB.AAANo ratings yet
- AXA Musculoskeletal QuestionnaireDocument2 pagesAXA Musculoskeletal QuestionnaireClaudine Limasa TabudlongNo ratings yet
- Senior Conference 2013 FormsDocument7 pagesSenior Conference 2013 FormsshamswayNo ratings yet
- PSRC Medical and Consent Form 20230727Document3 pagesPSRC Medical and Consent Form 20230727bigdog99bcNo ratings yet
- SKD Death Claim English Ver. 01Document1 pageSKD Death Claim English Ver. 01velandoNo ratings yet
- Maldives Medical and Dental Council: Application For Registration and Practising LicenseDocument4 pagesMaldives Medical and Dental Council: Application For Registration and Practising LicenseKamran FarooquiNo ratings yet
- Corporate Membership Application FormDocument2 pagesCorporate Membership Application Formpradhan13100% (1)
- Informed ConsentDocument2 pagesInformed Consentareebashaukat72No ratings yet
- 2022 Heart Screening Consent PacketDocument8 pages2022 Heart Screening Consent PacketBria GremillionNo ratings yet
- Medical Cer Ficate of Fitness: To Be Filled by CandidateDocument2 pagesMedical Cer Ficate of Fitness: To Be Filled by CandidateDINESH CHANDRA GANNAVARAPUNo ratings yet
- Admin Service Duty Travel Entry-Medical-Examination-Form MS-2Document7 pagesAdmin Service Duty Travel Entry-Medical-Examination-Form MS-2calistus wekesaNo ratings yet
- Apgenco 2012 Certificate of Fitness 22032012Document2 pagesApgenco 2012 Certificate of Fitness 22032012Veera ChaitanyaNo ratings yet
- Pak Takaful Claim FormDocument2 pagesPak Takaful Claim FormRoger Eli Paul100% (1)
- HTD Youth Camp Medical and Consent FormDocument2 pagesHTD Youth Camp Medical and Consent FormChris BowditchNo ratings yet
- Diabetes+mellitus+questionnaire ApplicantDocument2 pagesDiabetes+mellitus+questionnaire ApplicantClaudine Limasa TabudlongNo ratings yet
- Authorization For Release of Medical Information BSWHDocument1 pageAuthorization For Release of Medical Information BSWHCarrie FullerNo ratings yet
- One Step Med: General Medical Information Record Keeping ManualFrom EverandOne Step Med: General Medical Information Record Keeping ManualNo ratings yet
- Guide to Intellectual Disabilities: A Clinical HandbookFrom EverandGuide to Intellectual Disabilities: A Clinical HandbookJulie P. GentileNo ratings yet
- Hilton Head Relocation GuideDocument50 pagesHilton Head Relocation GuidebernardhhiNo ratings yet
- Julie Toon Pawley ResumeDocument1 pageJulie Toon Pawley Resumebernardhhi100% (1)
- Footloose Playbill FinalDocument6 pagesFootloose Playbill Finalbernardhhi100% (3)
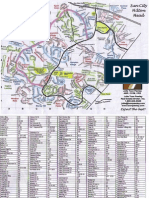
- Sun City Hilton Head Street Map-JTPDocument2 pagesSun City Hilton Head Street Map-JTPbernardhhi100% (3)
- Heroes On Horseback Summer 08 NewsletterDocument2 pagesHeroes On Horseback Summer 08 NewsletterbernardhhiNo ratings yet
- JanFeb 08 WebDocument16 pagesJanFeb 08 WebbernardhhiNo ratings yet
- Ladybird Book - The PolicemanDocument15 pagesLadybird Book - The Policemanbernardhhi91% (11)
- HOH Volunteer FormsDocument4 pagesHOH Volunteer FormsbernardhhiNo ratings yet
- Spring 2008 Continuing-Registration-FormDocument1 pageSpring 2008 Continuing-Registration-FormbernardhhiNo ratings yet
- Summer 2008 Continuing-Registration-FormDocument1 pageSummer 2008 Continuing-Registration-FormbernardhhiNo ratings yet
- Stay Safe: Teacher Resource Lessons 1 & 2Document7 pagesStay Safe: Teacher Resource Lessons 1 & 2Gary PhamNo ratings yet
- Aura Court - M15 4AB - Type 4 FRA - 19.02.19Document27 pagesAura Court - M15 4AB - Type 4 FRA - 19.02.19Noor Muddassir KhanNo ratings yet
- ACC-675 Week 3Document15 pagesACC-675 Week 3AllisonNo ratings yet
- Marble Project Feasibility in PakistanDocument10 pagesMarble Project Feasibility in PakistanSHAMANo ratings yet
- RM-No.-306-S.-2020 - TLE MELCDocument45 pagesRM-No.-306-S.-2020 - TLE MELCMilbert Awa-aoNo ratings yet
- Factory Automation Investment Thesis (SANITIZED)Document10 pagesFactory Automation Investment Thesis (SANITIZED)SSBCNo ratings yet
- Trust in E-Commerce PDFDocument7 pagesTrust in E-Commerce PDFSector VerdeNo ratings yet
- NSTP Bantilan FinalDocument10 pagesNSTP Bantilan Finaleleonor bantilanNo ratings yet
- Risk Assesment Template - ExcavationsDocument3 pagesRisk Assesment Template - ExcavationsPatrick MortNo ratings yet
- Geotechnical Risk in RailwaysDocument79 pagesGeotechnical Risk in RailwaysSergio Cunha100% (1)
- c6 Aud TheoryDocument11 pagesc6 Aud TheoryRachel Anne RascoNo ratings yet
- Smelter JudgementDocument206 pagesSmelter JudgementShavi Walters-SkeelNo ratings yet
- Risk Assessment MR-FRM-014, Rev 00Document10 pagesRisk Assessment MR-FRM-014, Rev 00rifaNo ratings yet
- Crisil Analysis 50 Leading SmesDocument64 pagesCrisil Analysis 50 Leading Smesflytorahul100% (1)
- Suicide and Mental HealthDocument3 pagesSuicide and Mental HealthAmar narayanNo ratings yet
- Work Camp Management Plan DraftDocument46 pagesWork Camp Management Plan Draftdinku yakobNo ratings yet
- Micro InsuranceDocument37 pagesMicro InsuranceBhavna Advani100% (2)
- Cemetery Guidance Northern IrelandDocument12 pagesCemetery Guidance Northern IrelandKelli FlorianiNo ratings yet
- 7 Test Plan Template Evaluation of Test Results Template and ExamplesDocument13 pages7 Test Plan Template Evaluation of Test Results Template and ExamplesSofa SofianaNo ratings yet
- DX031116 GSPR Atellica VTLi hs-cTnI Reagent V2Document48 pagesDX031116 GSPR Atellica VTLi hs-cTnI Reagent V2alexvo.1612No ratings yet
- A Comparison of Empirically Based and Structured Professional Judgment Estimation of Risk Using The Structured Assessment of Violence Risk in YouthDocument18 pagesA Comparison of Empirically Based and Structured Professional Judgment Estimation of Risk Using The Structured Assessment of Violence Risk in YouthDark SiriusNo ratings yet
- James Shore - The Art of Agile Development Assess Your AgilityDocument6 pagesJames Shore - The Art of Agile Development Assess Your AgilityDario FloresNo ratings yet
- Chapter 5: Fraud in Financial Statements and Auditor ResponsibilitiesDocument7 pagesChapter 5: Fraud in Financial Statements and Auditor ResponsibilitiesaaagamecockNo ratings yet
- Pai - Lecture3 - Measures of Disease FreqDocument53 pagesPai - Lecture3 - Measures of Disease FreqderieNo ratings yet