You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- BuffaloCheckQuiltPattern EmptyBobbinSewingStudioDocument3 pagesBuffaloCheckQuiltPattern EmptyBobbinSewingStudioMaria Mourão0% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Essential Elements of Piano TechniqueDocument24 pagesEssential Elements of Piano TechniqueMassimiliano Baggio83% (6)
- Curse of The PharaohDocument6 pagesCurse of The PharaohElysee TinTin MomplaisirNo ratings yet
- Common, Primordial, Giant Armour: None Weapons: Daggers, Darts, Slings, Quarterstaffs, Light Crossbows Tools: Poisoner's Kit 15Document3 pagesCommon, Primordial, Giant Armour: None Weapons: Daggers, Darts, Slings, Quarterstaffs, Light Crossbows Tools: Poisoner's Kit 15chrisNo ratings yet
- Football in The Blood by Tommy McLean Extract PDFDocument37 pagesFootball in The Blood by Tommy McLean Extract PDFBlack & White PublishingNo ratings yet
- Table Tennis Lesson Plan 1Document5 pagesTable Tennis Lesson Plan 1api-439899587No ratings yet
- New Microsoft Office Word DocumentDocument14 pagesNew Microsoft Office Word DocumentdrhalwagyNo ratings yet
- Role of Physical TherapistsDocument4 pagesRole of Physical TherapistsdrhalwagyNo ratings yet
- Role of Physical TherapistsDocument4 pagesRole of Physical TherapistsdrhalwagyNo ratings yet
- Rotator Cuff Shoulder Girdle TestsDocument2 pagesRotator Cuff Shoulder Girdle TestsdrhalwagyNo ratings yet
- 003Document33 pages003drhalwagyNo ratings yet
- Knee Injuries PH - Th.Document2 pagesKnee Injuries PH - Th.drhalwagyNo ratings yet
- Chapter 1 Sports Injury Management and The ATCDocument14 pagesChapter 1 Sports Injury Management and The ATCdrhalwagyNo ratings yet
- Use SO/NEITHER Auxiliary verbsDocument2 pagesUse SO/NEITHER Auxiliary verbslaura leitonNo ratings yet
- Game of KingsDocument2 pagesGame of KingsRuqiyya QayyumNo ratings yet
- 2018 All-State BaseballDocument1 page2018 All-State BaseballHonolulu Star-AdvertiserNo ratings yet
- Flywheel Ring GearDocument9 pagesFlywheel Ring Gearali42990% (1)
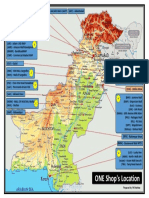
- One Shop's Location On Pakistan MapDocument1 pageOne Shop's Location On Pakistan MapMuhammad ToheedNo ratings yet
- Lethargic Weakness Decreased Performance: Nursing Care PlanDocument2 pagesLethargic Weakness Decreased Performance: Nursing Care PlanZhayree R.No ratings yet
- Mod ManagerDocument5 pagesMod ManagerAgnesthesiaNo ratings yet
- Rewritten Chronicles Manual V1 PDFDocument34 pagesRewritten Chronicles Manual V1 PDFPanNo ratings yet
- Lamborghini HuracánEVOSpyder AIDEMT 23.01.22Document17 pagesLamborghini HuracánEVOSpyder AIDEMT 23.01.22Aadit TuliNo ratings yet
- FINAL_FANTASY_XVI_Fact_Sheet_-_FINALDocument2 pagesFINAL_FANTASY_XVI_Fact_Sheet_-_FINALChristian MoratoNo ratings yet
- Train Flexibility and Strength for Higher Side KicksDocument12 pagesTrain Flexibility and Strength for Higher Side KicksTiago MinelliNo ratings yet
- Owner'S: ManualDocument19 pagesOwner'S: ManualValentin SerebrinskyNo ratings yet
- WindChart-Main Update 22.04.2022Document6 pagesWindChart-Main Update 22.04.2022Muhammad SyafiqNo ratings yet
- Club FootDocument104 pagesClub FootKittipong PoolketkitNo ratings yet
- Adidas IMC Final PresentationDocument14 pagesAdidas IMC Final PresentationBilawal Shabbir67% (3)
- 3000pts Ogre Kingdoms List v2 (Lizardmen) (HTML)Document8 pages3000pts Ogre Kingdoms List v2 (Lizardmen) (HTML)James NeunerNo ratings yet
- Physical Fitness EvaluationDocument60 pagesPhysical Fitness EvaluationMohd GjanNo ratings yet
- First Filipino on Everest? Dale Abenojar claims earlier summitDocument2 pagesFirst Filipino on Everest? Dale Abenojar claims earlier summitHarold Kim ValenzuelaNo ratings yet
- ESA Essential Facts 2015Document20 pagesESA Essential Facts 2015punter07No ratings yet
- Dominate Grail War Manual EnglishDocument20 pagesDominate Grail War Manual EnglishJoshuaNo ratings yet
- P90X/P90X2 Hybrid Workout SchedulesDocument3 pagesP90X/P90X2 Hybrid Workout SchedulesDragouilleNo ratings yet
- Monzo Bank Statement 2021 01 04 015938Document32 pagesMonzo Bank Statement 2021 01 04 01593813KARATNo ratings yet
- GbatekDocument1,426 pagesGbatekWen HuaNo ratings yet
- Enable VoLTE Oneplus 6Document2 pagesEnable VoLTE Oneplus 6weyigag657No ratings yet