You might also like
- Pleasure WomenDocument36 pagesPleasure WomenAsish ChakrabortyNo ratings yet
- Psychology IntroductionDocument75 pagesPsychology Introductionsanjivdas100% (1)
- 用-PSYCHOTHERAPYDocument103 pages用-PSYCHOTHERAPYsanjivdas100% (3)
- Hernia, (Different Types) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHernia, (Different Types) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Placental AbnormalitiesDocument42 pagesPlacental AbnormalitiesTee VillanuevaNo ratings yet
- Problems of The PassengerDocument9 pagesProblems of The PassengerDanah Grace SanchezNo ratings yet
- Legal Med - Ratio CompleteDocument25 pagesLegal Med - Ratio CompleteIS99057No ratings yet
- Abnormal Labor. BBBB WWPPTXDocument53 pagesAbnormal Labor. BBBB WWPPTXHamss Ahmed100% (2)
- Obstetrics and Gynecological InstrumentsDocument31 pagesObstetrics and Gynecological InstrumentsGAYATHRI RAKESHNo ratings yet
- Trans Women Safer Sex GuideDocument13 pagesTrans Women Safer Sex GuideLilith Dix0% (1)
- Genitalia AssessmentDocument99 pagesGenitalia AssessmentGloriaCoronado75% (8)
- Labor and DeliveryDocument128 pagesLabor and Deliveryalimk528950% (2)
- External HerniaDocument136 pagesExternal Herniasanjivdas100% (1)
- 2018my Zamala BreechmalpresentationDocument72 pages2018my Zamala BreechmalpresentationSaeed HasanNo ratings yet
- Lecture 17 Canine InfertilityDocument28 pagesLecture 17 Canine InfertilitygnpobsNo ratings yet
- Uterine Anomaly, Fibroid Uterus, Ovarian Tumor, Uterine ProlapseDocument30 pagesUterine Anomaly, Fibroid Uterus, Ovarian Tumor, Uterine ProlapseVijith.V.kumar80% (5)
- Breech DeliveryDocument6 pagesBreech DeliveryNyoman TapayanaNo ratings yet
- Abnormalities of Labour and Delivery and Their Management: Joó József GáborDocument44 pagesAbnormalities of Labour and Delivery and Their Management: Joó József GáborAnnisa Mutiara InsaniNo ratings yet
- ACOG Postpartum Discharge FormDocument2 pagesACOG Postpartum Discharge Formnandipati ramnadh100% (1)
- Breech PresentationDocument53 pagesBreech PresentationVijith.V.kumar100% (6)
- Abdul Hakeem Hady.: Done byDocument29 pagesAbdul Hakeem Hady.: Done byعمر احمد شاكرNo ratings yet
- Normal Labor and DeliveryDocument61 pagesNormal Labor and DeliverySulistianto TianNo ratings yet
- POP June 10,2021 1Document48 pagesPOP June 10,2021 1Kerod AbebeNo ratings yet
- Refarat Ginekologi - Prolaps Organ PanggulDocument29 pagesRefarat Ginekologi - Prolaps Organ Panggullhia priscillaNo ratings yet
- Anorectal Malformations: Richard J. Wood, MD Marc A. Levitt, MDDocument10 pagesAnorectal Malformations: Richard J. Wood, MD Marc A. Levitt, MDsuci triana putriNo ratings yet
- Physiology of LabourDocument40 pagesPhysiology of LabourShubhi VaivhareNo ratings yet
- 5 - DystociaDocument43 pages5 - DystociaMara Medina - BorleoNo ratings yet
- GlaucomaDocument23 pagesGlaucomasanjivdas100% (2)
- Nursing Care Plan For Labor and Delivery Stages of Labor Diagnosis Intervention Rationale IndependentDocument7 pagesNursing Care Plan For Labor and Delivery Stages of Labor Diagnosis Intervention Rationale IndependentCLARISSE GEMROSE CUÑADANo ratings yet
- 9 The Post Anesthesia Care UnitDocument77 pages9 The Post Anesthesia Care Unitsanjivdas100% (1)
- Normal Labor and DeliveryDocument97 pagesNormal Labor and DeliveryAwee Wee100% (1)
- Uterine Abnormality and DisplacementDocument29 pagesUterine Abnormality and DisplacementKinjal Vasava100% (4)
- 3 Problems With The Passenger and Powers of LaborDocument105 pages3 Problems With The Passenger and Powers of LaborRaquel M. MendozaNo ratings yet
- Bias and ConfoundingDocument27 pagesBias and ConfoundingsanjivdasNo ratings yet
- Bias and ConfoundingDocument27 pagesBias and ConfoundingsanjivdasNo ratings yet
- Answer of Exercises-Measures of Disease FrequencyDocument7 pagesAnswer of Exercises-Measures of Disease Frequencysanjivdas100% (4)
- GRAND PRES - CorrectedDocument22 pagesGRAND PRES - CorrectedDarlen RabanoNo ratings yet
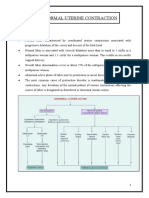
- Abnormal Uterine ContractionDocument34 pagesAbnormal Uterine Contractionsapana shahNo ratings yet
- Contracted Pelvis: Rupture of The UterusDocument42 pagesContracted Pelvis: Rupture of The UterusMed PoxNo ratings yet
- Pathological DeliveryDocument44 pagesPathological DeliverySitti AraNo ratings yet
- Obstructed LaborDocument41 pagesObstructed LaborHenok Y KebedeNo ratings yet
- Difficult Labor (Dystocia) : Disproportion Between The Presenting Part of The Fetus and The Birth CanalDocument9 pagesDifficult Labor (Dystocia) : Disproportion Between The Presenting Part of The Fetus and The Birth CanalMohammad Hadi AlghuraifiNo ratings yet
- Class SssssssDocument34 pagesClass SssssssPrajwal ChhetriNo ratings yet
- Introduce Myself: Chinese Name: English Name: Dong Dirong Profession: Obstetrics and Work In: Zhongnan HospitalDocument80 pagesIntroduce Myself: Chinese Name: English Name: Dong Dirong Profession: Obstetrics and Work In: Zhongnan Hospitalapi-19641337No ratings yet
- LP Prolpase Uterin - Id.en InggrisDocument13 pagesLP Prolpase Uterin - Id.en InggrisNajahNo ratings yet
- 09 Abnormalities Labor-FqlDocument50 pages09 Abnormalities Labor-Fqlapi-19916399No ratings yet
- Malposition & Malpresentation: Ahmad MakhloufDocument72 pagesMalposition & Malpresentation: Ahmad Makhloufjssamc prasootitantraNo ratings yet
- Hands Out 3 LaborDocument29 pagesHands Out 3 LaborErin SaavedraNo ratings yet
- Congenital Diaphragmatic HerniaDocument3 pagesCongenital Diaphragmatic HerniaMahmoud SalmanNo ratings yet
- Breech-Presentation (2) - 1Document30 pagesBreech-Presentation (2) - 1ahmed shorshNo ratings yet
- Benign Cervical Lesions and Congenital Anomalies of The Cervix - UpToDateDocument33 pagesBenign Cervical Lesions and Congenital Anomalies of The Cervix - UpToDatecriswesi23No ratings yet
- Abdominal Wall Hernias Comprehensive Gynecology Anatomic Defects ofDocument1 pageAbdominal Wall Hernias Comprehensive Gynecology Anatomic Defects ofPia FerrarisNo ratings yet
- Early Pregnancy Complications: by Harvir Singh Supervised by DR Ranjit and DR SyafiqahDocument33 pagesEarly Pregnancy Complications: by Harvir Singh Supervised by DR Ranjit and DR SyafiqahShre RanjithamNo ratings yet
- Breech PresentationDocument83 pagesBreech Presentation9446228080No ratings yet
- DR - Ayman MalpresentationDocument21 pagesDR - Ayman MalpresentationJalajarani AridassNo ratings yet
- Breech PresentationDocument85 pagesBreech Presentationwidya vannesaNo ratings yet
- Abnormaluterineaction 190228112826Document62 pagesAbnormaluterineaction 190228112826James MainaNo ratings yet
- Etal Osition and ResentationDocument32 pagesEtal Osition and ResentationJennifer Samuel SinghNo ratings yet
- Breech Presentation-Pritiss Nair Group 2Document45 pagesBreech Presentation-Pritiss Nair Group 2asmeralda99No ratings yet
- Femoral HerniaDocument3 pagesFemoral HerniakhurshidghorihumaNo ratings yet
- 05 DystociaDocument10 pages05 DystociaRiantiara PutrizaNo ratings yet
- Content WriterDocument51 pagesContent WriterToday ViralNo ratings yet
- 012 090 Groin HerniaDocument8 pages012 090 Groin HerniaxcalibursysNo ratings yet
- High Risk LabourDocument38 pagesHigh Risk LabourprakruthiNo ratings yet
- Ectopic Pregnancy 2022 Edited 3Document40 pagesEctopic Pregnancy 2022 Edited 3apule geraldhumbleNo ratings yet
- Obstructed LabourDocument5 pagesObstructed LabourswethashakiNo ratings yet
- Inguinal Hernia: From Wikipedia, The Free EncyclopediaDocument6 pagesInguinal Hernia: From Wikipedia, The Free EncyclopediaSherlyn YeeNo ratings yet
- Gynecologic-Nursing Part 2Document40 pagesGynecologic-Nursing Part 2jomariNo ratings yet
- Abnormal Uterine Actions - Monika MakwanaDocument10 pagesAbnormal Uterine Actions - Monika Makwanamonika makwanaNo ratings yet
- Hysterosalpingography (HSG) Anatomy, Imaging and Pathology RevisitedDocument16 pagesHysterosalpingography (HSG) Anatomy, Imaging and Pathology Revisitedgrahapuspa17No ratings yet
- HerniaDocument47 pagesHerniamalathiNo ratings yet
- I Group of Questions 1Document31 pagesI Group of Questions 1siwap34656No ratings yet
- 30 - Contracted Pelvis and Cephalopelvic DisproportionDocument28 pages30 - Contracted Pelvis and Cephalopelvic Disproportiondr_asaleh93% (14)
- Ectopic PregnancyDocument76 pagesEctopic PregnancyVivian Jean TapayaNo ratings yet
- Abnormal Uterine ActionDocument32 pagesAbnormal Uterine ActionSona amoreux De JESUSNo ratings yet
- Ante Partum HemorrhageDocument21 pagesAnte Partum HemorrhagejyothinanduriNo ratings yet
- Abnormal LabourDocument7 pagesAbnormal LabourSaman SarKo0% (1)
- Anomalies of The Female Genital TractDocument2 pagesAnomalies of The Female Genital TractAnastasia KasapiNo ratings yet
- Complications During Labor and Delivery: I. Dysfunctional Labor A. DystociaDocument16 pagesComplications During Labor and Delivery: I. Dysfunctional Labor A. DystociaEden NatividadNo ratings yet
- Acute Suppurative PeritonitisDocument47 pagesAcute Suppurative PeritonitissanjivdasNo ratings yet
- Female Genital TumorDocument55 pagesFemale Genital TumorsanjivdasNo ratings yet
- Leiomyoma of The UterusDocument17 pagesLeiomyoma of The UterussanjivdasNo ratings yet
- Chronic Renal FailureDocument54 pagesChronic Renal Failuresanjivdas100% (3)
- Chapter 1 Signs and Symptoms of Mental DisordersDocument120 pagesChapter 1 Signs and Symptoms of Mental DisorderssanjivdasNo ratings yet
- Urinarytract InfectionDocument61 pagesUrinarytract InfectionsanjivdasNo ratings yet
- 28-Randomised Controlled Trial-YangBF 09.5.12Document14 pages28-Randomised Controlled Trial-YangBF 09.5.12sanjivdasNo ratings yet
- This Is Extremely Difficult To Detect Yourself: Optic NerveDocument4 pagesThis Is Extremely Difficult To Detect Yourself: Optic NervesanjivdasNo ratings yet
- Disorders of The Urinary System General IntroductionDocument63 pagesDisorders of The Urinary System General IntroductionsanjivdasNo ratings yet
- 8 Stress and Coping: Jining Medical College Department of Psychology Ji FengDocument44 pages8 Stress and Coping: Jining Medical College Department of Psychology Ji FengsanjivdasNo ratings yet
- Glaucoma: Information and TreatmentDocument22 pagesGlaucoma: Information and TreatmentsanjivdasNo ratings yet
- Congenital Heart Disease 1223958712449685 9Document58 pagesCongenital Heart Disease 1223958712449685 9RinaNo ratings yet
- Unintentional Trauma During Gynaecological Surgery: I. Z. MackenzieDocument8 pagesUnintentional Trauma During Gynaecological Surgery: I. Z. Mackenziemuhammadnurul asmiNo ratings yet
- MetrorrhagiaDocument24 pagesMetrorrhagiaMatt SarigumbaNo ratings yet
- CH 13 Microbe-Human Interactions (Student) .PPT (Compatibility Mode)Document12 pagesCH 13 Microbe-Human Interactions (Student) .PPT (Compatibility Mode)shanika100% (1)
- IndianJObstetGynecolRes 9 2 198 203Document6 pagesIndianJObstetGynecolRes 9 2 198 203shilpi sumanNo ratings yet
- Female Sexualexperience Lessons Learned From Expert Interviews AuthorDocument30 pagesFemale Sexualexperience Lessons Learned From Expert Interviews AuthorUvaçinNo ratings yet
- Chapter 5 (Maternal)Document47 pagesChapter 5 (Maternal)Veloria AbegailNo ratings yet
- LacerationsDocument2 pagesLacerationsGoldyNo ratings yet
- Group 3 - PCOS and SD Written OutputDocument25 pagesGroup 3 - PCOS and SD Written OutputJolly S. SendinNo ratings yet
- Ovarian New GrowthDocument215 pagesOvarian New GrowthKaissa GomezNo ratings yet
- HIV Transmission FAQsDocument8 pagesHIV Transmission FAQsbaradiNo ratings yet
- (Ob1) 1.02 - History and Physical Exam - Dr. NicanorDocument7 pages(Ob1) 1.02 - History and Physical Exam - Dr. NicanorJakeNo ratings yet
- Postnatal Exercises: Caring For Your BodyDocument16 pagesPostnatal Exercises: Caring For Your BodyLga PrakashNo ratings yet
- Post Coital BleedingDocument8 pagesPost Coital BleedingMutiara SwNo ratings yet
- 2 - Puberty-GirlsDocument40 pages2 - Puberty-Girlsapi-241585431No ratings yet
- Vaginal DischargeDocument1 pageVaginal DischargeVidini Kusuma AjiNo ratings yet
- Abnormal Uterine BleedingDocument10 pagesAbnormal Uterine BleedingHaryoko AnandaputraNo ratings yet
- DewgardenDocument14 pagesDewgardenpushpa100% (4)
- Lecture Notes AnatomyDocument18 pagesLecture Notes AnatomyFau Fau DheoboNo ratings yet