Cardiovascular System
BY: Rolinette Dane G. Cruz Aileen Chavez
�CARDIOVASCULAR SYSTEM
ANATOMY AND PHYSIOLOGY Composed of the heart and Composed of the vascular system
MAJOR FUNCTION OF CARDOVASCULAR SYSTEM Transporting nutrients and oxygen to the body Removing wastes and carbon dioxide Maintaining adequate perfusion of organs and tissues
�VASCULAR SYTSYEM
Is composed of the blood vessels of the body The blood vessel of the body have 3 types: Arteries (arterioles) Veins (venules) Capillaries
�BLOOD VESSEL
Arteries (and arterioles) Are large, thick-walled muscular vessels that carry blood away from the heart The largest artery is the aorta. The middle layer of an artery wall consists of smooth muscle that can constrict to regulate blood flow and blood pressure. Arterioles can constrict or dilate, changing blood pressure. Veins (and venules) large blood vessels that carry blood from the tissues back to the heart Venules drain blood from capillaries, then join to form veins that take blood to the heart.
� Veins have much less smooth muscle and connective tissue than arteries.
Veins often have valves that prevent the backward flow of blood when closed. Veins carry about 70% of the bodys blood and act as a reservoir during hemorrhage.
� Capillaries
Are microscopic blood vessels with walls that are only one cell thick to enable nutrients and gases to diffuse easily between blood and tissues Capillaries have walls only one cell thick to allow exchange of gases and nutrients with tissue fluid. Capillary beds are present in all regions of the body but not all capillary beds are open at the same time. Contraction of a sphincter muscle closes off a bed and blood can flow through an arteriovenous shunt that bypasses the capillary bed.
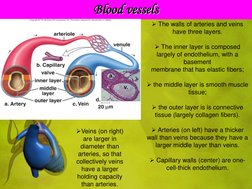
�Blood vessels
The walls of arteries and veins have three layers. The inner layer is composed largely of endothelium, with a basement membrane that has elastic fibers; the middle layer is smooth muscle tissue; the outer layer is is connective tissue (largely collagen fibers). Veins (on right) are larger in diameter than arteries, so that collectively veins have a larger holding capacity than arteries. Arteries (on left) have a thicker wall than veins because they have a larger middle layer than veins. Capillary walls (center) are onecell-thick endothelium.
�HEART
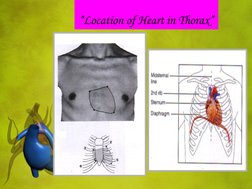
Lying between lungs and middle mediastinum.
Four chambered, hollow muscular organ.
Size of mans fist. Base directed upward/ apex downward to the left Covered by fibroserous sac- PERICARDIUM
TWO LAYER
Inner Visecral Pericardium =lines the surface of the heart Outer Parietal Pericardium = fluid between the serous and fibrous = lubricates the layers and allows for a gliding
motion between them w/ each heartbeat
�Location of Heart in Thorax
� 4 CHAMBER OF THE HEART
1. Right Atrium
Larger than the left
Walls are thin
2. Left Atrium Have a thicker walls than the right Receives blood from lungs by way of for pulmonary vasculature Mitral orifice- guarded by MITRAL VALVE
3.Right Ventricle
Constitutes right inferior portion of apex of the heart. Receives blood from right atrium(RA) and brings blood to The lungs trought the PULMONARY ARTERIES.
� Inner surface the muscular column = TROBECULAE CARNAE. Some muscular colums project and called = PAPILLARY MUSCLES. At ends papillae are fibrous strancolled CHORDAE TENDINAE- keeps valve leaf lets from turning out.
Pulomonary orifice- guarded by pulmonary valve Tricuspid orifice- guarded by tricuspid balve 4. Left Ventricle Constitute left inferior portion of the apex of the heart
thick walls =pumps blood received from left atrium (LA) of the blood through the aorta
RIGHT AND VENTRICLES = separated by Intervenricular Septum
�3 VEINS EMPTY INTO RIGHT ATRIUM (RA)
1. Superior Vena Cava( SVC)
Brings blood from upper portions of body 2. Inferior Vena Cava(IVC) Brings blood from lower part of the body 3. Coronary Sinus Drains blood from the heart itself
�External heart anatomy
The superior vena cava and the pulmonary trunk are attached to the right side of the heart.
The aorta and pulmonary veins are attached to the left side of the heart. The right ventricle forms most of the ventral surface of the heart, and the left ventricle forms most of the dorsal surface
�Coronary artery circulation
The coronary arteries and cardiac veins pervade cardiac muscle.
The coronary arteries bring oxygen and nutrients to cardiac cells, which derive no benefit from blood coursing through the heart.
�VALVES OF THE HEART
1.
ATRIOVENTRICULAR VALVES OR AV VALVES A. TRICUSPID prevents backflow of blood from right ventricle(RV) to right atrium( RA)
B.MITRAL OR BICUSPID Prevents backflow of blood from left ventricle(LV) to left atrium(LA)
2. SEMILUNAR VALVES
A.PULMONARY Prevents backflow of blood from pulmonary arteries( PA)
B.AORTIC Prevents backflow of blood from aorta
�Passage of Blood Through the Heart
Blood follows this sequence through the heart: superior and inferior vena cava right atrium tricuspid valve right ventricle pulmonary semilunar valve pulmonary trunk and arteries to the lungs pulmonary veins leaving the lungs left atrium bicuspid valve left ventricle aortic semilunar valve aorta to the body.
�WALLS OF THE HEART 3 LAYERS
1. EPICARDIUM - from Greek; epi- outer, cardium heart
Outer layer- fibers b.v & nerves
2. MYOCARDIUM
Middle muscular layer Heart muscular contracts rhythmically and spontaneously
3. ENDOCARDIUM Innermost layer = collagenous, elastin fibers b.v, and nerves and purkinje fibers
� WALLS OF THE HEART 3- LAYERS
1.
SINO-ATRIAL NODE (SA NODE) Located post wall of right atrium (RA) Initiates heartbeat- ( CARDIAC PACEMAKER)
2. ATRIO-VENTRICULAR NODE ( AV-NODE) Located right side of inter atrial septum There is a delay in the conduction of excitation at the A NODE to allow time for a the atria to complete the emptying of their contest to the ventricles 3. BUNDLE OF HIS OR ANTRIOVENTRICULAR BUNDLES (AV BUNDLES) Goes down to the right side of inter-ventricular septum and divides into a right and left branches. Each branches divides into conducting fibers known as PURKINJE FIBERS from antrioventricular node (AV node) excitation spreads through the bundles of his 4. PURKENJE FIBERS Conducting fibers of left and right branches of the bundle of his extends over to the undersurface of endocardium
�Conduction system of the heart
The SA node sends out a stimulus, which cause the atria to contract. When this stimulus reaches the AV node, it signals the ventricles to contract. Impulses pass down the two branches of the atrioventricular bundle to the Purkinje fibers, and thereafter the ventricles contract.
OUTLINE CONDUCTING SYSTEM
Sino-Atrial node (SA NODE)
Atrio-Ventricular node (AV-NODE) NODE)
Right branch
Left branch
Purkinje fibers
Purkinje fibers
�Internal view of the heart
The heart has four valves. The atrioventricular valves allow blood to pass from the atria to the ventricles, and the semilunar valves allow blood to pass out of the heart.
� The pumping of the heart sends out blood under pressure to the arteries.
Blood pressure is greatest in the aorta; the wall of the left ventricle is thicker than that of the right ventricle and pumps blood to the entire body.
Blood pressure then decreases as the cross-sectional area of arteries and then arterioles increases.
�Path of blood through the heart
This diagrammatic
representation of the heart allows you to trace the path of the blood through the heart.
�The Vascular Pathways
The cardiovascular system includes two circuits:
1) Pulmonary circuit which circulates blood through the lungs, and
The pulmonary circuit begins with the pulmonary trunk from the right ventricle which branches into two pulmonary arteries that take oxygen-poor blood to the lungs. In the lungs, oxygen diffuses into the blood, and carbon dioxide diffuses out of the blood to be expelled by the lungs. Four pulmonary veins return oxygen-rich blood to the left atrium.
�2) Systemic circuit which circulates blood to the rest of the body.
The systemic circuit starts with the aorta carrying O2rich blood from the left ventricle. The aorta branches with an artery going to each specific organ. Generally, an artery divides into arterioles and capillaries which then lead to venules.
� The vein that takes blood to the vena cava often has the same name as the artery that delivered blood to the organ. In the adult systemic circuit, arteries carry blood that is relatively high in oxygen and relatively low in carbon dioxide, and veins carry blood that is relatively low in oxygen and relatively high in carbon dioxide. This is the reverse of the pulmonary circuit.
3) Both circuits are vital to homeostasis.
�Major arteries and veins of the systemic circuit
A realistic representation of the major blood vessels of the systemic circuit shows how the systemic arteries and veins are arranged in the body.
� The coronary arteries serve the heart muscle itself; they are the first branch off the aorta. Since the coronary arteries are so small, they are easily clogged, leading to heart disease.
The hepatic portal system carries blood rich in nutrients from digestion in the small intestine to the liver, the organ that monitors the composition of the blood.
�Blood Flow
The beating of the heart is necessary to homeostasis because it creates pressure that propels blood in arteries and the arterioles.
Arterioles lead to the capillaries where nutrient and gas exchange with tissue fluid takes place.
�Cardiovascular system diagram
The blue-colored vessels carry O2-poor blood, and the red-colored vessels carry O2-rich blood; the arrows indicate the flow of blood. Capillaries are present in all parts of the body, so no cell is located far from a capillary.
�ASSESSMENT OF CARDIOVASCULAR SYSTEM
Equipment needed:
Blood Pressure
A watch w/ a second hand
Stethoscope w/ diaghram & bell
�CONT. EQUIPMENT NEEDED
Patient gown
�ASSESSMENT OF CARDIOVASCULAR SYSTEM
OBJECTIVES: 1. Describe the structure and function of cardiovascular system, including the pheripheral vascular system 2.Explain developmental variations a nurse considers when assessing the heart & neck vessels & pheripheral vascular system 3.State the specific areas considered essential in gathering subjective data pertaining to the cardiovascular system and the peripheral vascular system 4.Demonstrate assessment of the heart, neck vessels and pulmonary vein (PV) system
�4 TECHNIQUES
Cardiovascular examination
THE HEART (PRECORDIUM)
Inspection
Check pulsation, heaves, lifts, ( you may see the apical pulse) NOTE: The apical is located in the 4th or 5th intercostal space at the left midclavicle
Palpate
Feel the apical impulse. Use 1 finger pad Use palmar side of 4 fingersto feel for other pulsations on the chest (eg. Thrill)
PERCUSSION
To check for heart enlargement (Note : Often done by chest X-ray)
AUSCULTATION
Start of the base of the heart
APE Man
Aortic-2nd Rt ICS
Pulmonic-2nd left ICS
Erbs Point
Tricuspid left sternal border
Mitral-5th ICS at left midclavicle level
� DIFFERENT SOUND OF LUNG AUSCULTATION
BREATH SOUND:
NORMAL BREATH SOUND
1. Bronchial Sounds
They are normally heard over the trachea and larynx An I:E Ratio : 1:1 or 1:1 1/4 with a pause in between inspiration & expiration Thoracic Geography : over the manubrium of the sternum Sound Characteristics : high pitched, tubular, hollow sound Indication : pneumonia, atelectasis, fluid infiltration
ABNORMAL BREATH SOUND
1. Crackles
explosive, "popping" sounds that originate within the airways. They are heard when an obstructed airway suddenly opens and the pressures on either side of the obstruction suddenly equilibrates resulting in transient, distinct vibrations in the airway wall. The dynamic airway obstruction can be caused by either accumulation of secretions within the airway lumen or by airway collapse caused by pressure from inflammation or edema in
�Cont. Different of lung ascultation
NORMAL BREATH SOUND
2. Bronchovesicular Sounds consist of a full inspiratory phase with a shortened and softer expiratory phase They are normally heard over the hilar region in most resting animals and should be quieter than the tracheal breath sounds. However, in sheep, goats, llamas, and alpacas, they may be heard throughout the full lung field and are often louder than tracheal breath sounds. Increased intensity of bronchovesicular sounds is most often associated with increased ventilation or pulmonary consolidation.
ABNORMAL BREATH SOUND
can be heard during inspiration when intrathoracic negative pressure results in opening of the airways or on expiration when thoracic positive pressure forces collapsed or blocked airways open are heard more commonly during inspiration than expiration. They are significant as they imply either 2. Wheezes are continuous musical tones that are most commonly heard at end inspiration or early expiration.
�NORMAL BREATH SOUND
3. Vesicular Sounds consist of a quiet, wispy inspiratory phase followed by a short, almost silent expiratory phase. They are heard over the periphery of the lung field An I:E Ratio : 1:0 or 1:1/4 with no pause in between inspiration & expiration Thoracic Geography : everywhere on the thoracic wall Sound Characteristics : low pitched, soft rustling sound Indication : pneumonia, atelectasis, fluid infiltration
ABNORMAL BREATH SOUND
They result as a collapsed airway lumen gradually opens during inspiration or gradually closes during expiration As the airway lumen becomes smaller, the air flow velocity increases resulting in harmonic vibration of the airway wall and thus the musical tonal quality. can be classified as either high pitched or low pitched wheezes may be monophonic (a single pitch and tonal quality heard over an isolated area) or polyphonic (multiple pitches and tones heard over a variable area of the lung) significant as they imply decreased airway lumen diameter either due to thickening of reactive airway walls or collapse of airways due to pressure from surrounding pulmonary disease.
�NORMAL BREATH SOUND
ABNORMAL BREATH SOUND 3. Stridor
are intense continuous monophonic wheezes heard loudest over extrathoracic airways. They tend to be accentuated during inspiration when extrathoracic airways collapse due to lower internal lumen pressure. They can often be heard without the aid of a stethoscope. Careful auscultation with a stethoscope can usually identify an area of maximum intensity that is associated with the airway obstruction. This is typically either at the larynx or at the thoracic inlet.
�NORMAL BREATH SOUND
ABNORMAL BREATH SOUND
These extrathoracic sounds are often referred down the airways and can often be heard over the thorax and are often mistaken as pulmonary wheezes is significant and indicates upper airway obstruction.
4. Stertor is a poorly defined and inconsistently used term to describe harsh discontinuous crackling sounds heard over the larynx or trachea.
It is also described as a sonorous snoring sound heard over extrathoracic airways.
�NORMAL BREATH SOUND
ABNORMAL BREATH SOUND
Stertor does not have the musical quality of stridor
is significant as it is suggestive of accumulation of secretions within extrathoracic airways.
SEQUENCE FOR AUSCULATING
A. Begin with the diaphragm
Note at each area: 1.rate and rhythm 2. identify S1 and S2
3. Assess S1 and S2 separtely
4. listen for extra heart sound (ie. S3 and S4) 5. listen for murmur B. Repeat above using a bell
�ASSESSMENT OF THE HEART
HISTORY AND CURRENT STATUS QUESTION PERSONAL HISTORY OF CARDIAC DISEASE Congenital defect is a defect in the structure of the heart and great vessels of a newborn. is a defect in the structure of the heart and great vessels of a newborn. Most heart defects either obstruct blood flow in the heart or vessels near it or cause blood to flow through the heart in an abnormal pattern, although other defects affecting heart rhythm (such as long QT syndrome) can also occur.
Heart defects are among the most common birth defects and are the leading cause of birth defect-related deaths. Approximately 1 in 125 babies are born each year in the US with a Congenital Heart Defect.
Enlarge Heart is an increase in the size of the heart
may be caused by a thickening of the heart muscle because of increased workload. (This increased workload can be due to heart valve disease or high blood pressure,) This is called hypertrophy (hi-PER'tro-fe), which refers to enlargement of an organ or tissue due to an increase in cell size.
� Arrhythmias Heart
is a disorder of the heart rate (pulse) or heart rhythm, such as beating too fast (tachycardia), too slow (bradycardia), or irregularly. Arrhythmias may also be caused by some substances or drugs, including: Amphetamines Caffeine Cocaine Beta blockers Psychotropics Sympathomimetics
� Murmur
are extra heart sounds that are produced as a result of turbulent blood flow that is sufficient to produce audible noise. Most murmurs can only be heard with the assistance of a stethoscope ("on auscultation"). A functional murmur or "physiologic murmur" is a heart murmur that is primarily due to physiologic conditions outside the heart, as opposed to structural defects in the heart itself Functional murmurs may be benign (an "innocent murmur") mildly troublesome, or serious.
Congestive Heart Failure is a condition in which the heart can't pump enough blood to the body's other organs. This can result from: narrowed arteries that supply blood to the heart muscle coronary artery disease past heart attack, or myocardial infarction, with scar tissue that interferes with the heart muscle's normal work high blood pressure heart valve disease due to past rheumatic fever or other causes primary disease of the heart muscle itself, called cardiomyopathy. infection of the heart valves and/or heart muscle itself endocarditis and/or myocarditis heart defects present at birth congenital heart defects.
� Septal defect
a congenital abnormality in the septum
between the left and right sides of the heart Ventricular Septal Defect (VSD)
is a defect in the septum between the right and left ventricle.
The septum is a wall that separates the hearts left and right sides. Septal defects are sometimes called a hole in the heart.
Its the most common congenital heart defect in the newborn; its less common in older children and adults because some VSDs close on their own.
� Atrial Septal Defect (ASD) is a defect in the septum between the hearts two upper chambers (atria). The septum is a wall that separates the hearts left and right sides. Septal defects are sometimes called a hole in the heart.
�Angina or Myocardiac Infarction commonly known as a heart attack, is the interruption of blood supply to part of the heart, causing heart cells to die. This is most commonly due to occlusion (blockage) of a coronary artery following the rupture of a vulnerable atherosclerotic plaque, which is an unstable collection of lipids (fatty acids) and white blood cells (especially macrophages) in the wall of an artery
The resulting ischemia (restriction in blood supply) and oxygen shortage, if left untreated for a sufficient period of time, can cause damage or death (infarction) of heart muscle tissue (myocardium).
1. FAMILY HISTORY OF CARDIAC DISEASE Family members w/ any of the above described illnesses relation to the patient, specific problem, age of onset, age of death, disease/ cause of relatives death
2. RISKS FACTORS? Congenital heart Disease
is a type of defect or malformation in one or more structures of the heart or blood vessels that occurs before birth
� Rheumatic Fever is an inflammatory disease that occurs following a Group A streptococcal infection, (such as strep throat or scarlet fever). Believed to be caused by antibody cross-reactivity that can involve the heart, joints, skin, and brain, the illness typically develops two to three weeks after a streptococcal infection. Acute rheumatic fever commonly appears in children between the ages of 5 and 15, with only 20% of first-time attacks occurring in adults. The illness is so named because of its similarity in presentation to rheumatism.[2]
� Thyroid Disease
is a medical condition impairing the function of the thyroid. is a small gland located below the skin and muscles at the front of the
neck, just at the spot where a bow tie would rest.
Diabetes is classed as a metabolism disorder. Metabolism refers to the way our bodies use digested food for energy and growth.
Most of what we eat is broken down into glucose. Glucose is a form of sugar in the blood - it is the principal source of fuel for our bodies.
Obesity
is a medical condition in which excess body fat has accumulated to the extent that it may have an adverse effect on health, leading to reduced life expectancy and/or increased health problems
� Tobacco use
Smoking is a practice where a substance, most commonly tobacco, is burned and the smoke tasted or inhaled. .
Hypercholesterolemia
Hypercholesterolemia (literally: high blood cholesterol) is the presence of high levels of cholesterol in the blood. It is not a disease but a metabolic derangement that can be secondary to many diseases and can contribute to many forms of disease, most notably cardiovascular disease. It is closely related to the terms "hyperlipidemia" (elevated levels of lipids) and "hyperlipoproteinemia" (elevated levels of lipoproteins).
� Excessive caffeine
found naturally in tea and coffee plants which acts as a mild stimulant of the central nervous system
There are several short-term effects of caffeine. Some of the most common short-term effects of drinking caffeine are: increased alertness (caffeine is a mild stimulant) makes your heart beat faster (caffeine is a mild stimulant) makes you go to the toilet more (caffeine is a diuretic) raises your body temperature makes your digestive system produce
more acid.
� Alcohol or drug abuse Alcoholism is drinking alcoholic beverages at a level that interferes with physical health, mental health, and social, family, or job responsibilities.
� 3. CHEST PAIN? Often patients are unable to describe the sensation they feels as pain Can arise suddenly or gradually, and its cause may be difficult to ascertain initially.
The pain can radiate to the arms, neck, jaw, or back. It can be steady or intermittent, mild or acute
� 4.RHYTHM IRREGULARITIES? Are there palpatations Skipped beats Racing of the heart: when, how often; associated symptoms (shortness of breath, chespain or diaphoresis 5 .CYANOSIS? blue lips or nailbed Ashen color of skin Hacking, constant,intermittent, or rare; time of the day (e.g, early morning) Chest pain Productive or non productive: color and consistency of the sputum ( thick,thin, clear, yellow, green,maldorous, blood
tinged
�5. COUGH?
Hacking, constant,intermittent, or rare; time of the day (e.g, early morning) Chest pain Productive or non productive: color and consistency of the sputum (thick,thin,clear,yellow,green,maldorous, blood tinged) 6.FATIGUE? Ability to keep up w/ friends and colleagues
Sudden or gradual onset
Related to time of day
�7. EDEMA?
Where and when: lower legs Ankles;at night in the morning; pitting or non pitting; Unilateral or bilateral
Any associated pain
8. Nocturia?
Date of onset Number of times each night Waking at night w/ urgent need to urinate
�9. OCCUPATIONAL RISKS?
Stressful occupational Exposed to smoke Pollution Toxins Vapors Fumes Strenous excercise
�10. MEDICATION? Cardiovascular medications:
Type Dosage How long Side effects Any recent changes in medication or dosages
�11. PAS TWORK-UP? past cardiovascular test or surgery: Chest x-ray ECG Echocardiogram Exercise stress test Holter monitor Cardiac catherization Angiosplasty Valvuloplasty Valve replacement or bypass Results Complications
�HEART EXAMINATION
Holter monitoring
�Cont. heart examination
Chest x-ray
�cont. heart examination
Ecocardigram (ecg)
�cont.heart examination
angioplasty
�cont.heart examination
Valvuloplasty
�cont.heart examination
Cardiac catherization
�cont.heart examination
Valve replacement or bypass
�12. SHORTNESS OF BREATH?
Does it occur unexpectedly Is it constant or intermittent It occur at rest or with exertion? What type and how much activity provokes it Has this amount changed over time Occur at night Awaken patient from sleep Cause need for extra pillows Associated w/ cough Fever Chest pain or diaphoresis
�The Heartbeat
Each
heartbeat is called a cardiac cycle. When the heart beats, the two atria contract together, then the two ventricles contract; then the whole heart relaxes.
�CARDIAC CYCLE
IT HAS TWO PHASE:
1. SYSTOLIC
hearts contracts & pushes blood out of the ventricle to:
i.
The lungs
ii. Systemic arteries
2. DIASTOLE
Ventricles relax & filled with blood ( this 2/3 of the cardiac cycle)
� Extrinsic Control of Heartbeat
A cardiac control center in the medulla oblongata speeds up or slows down the heart rate by way of the autonomic nervous system branches: parasympathetic system (slows heart rate) and
the sympathetic system (increases heart rate).
Hormones epinephrine and norepinephrine from the adrenal medulla also stimulate faster heart rate.
HEART SOUNDS
S1
When closure of the Atrio-venricular (AV) Valves (tricuspid & mitral) & ventricles contract
�Cont. heart sound
S2
When closure of the semilunar valves (pulmonic & aortic) and the ventricles relax
�What do you hear?
S1 and S2 sound lub dup S1 and louder than S2 at the apex S2 is louder than S1 at the base S1 coincides w/ the carotid pulsation
�EXTRA HEART SOUNDS
S3 This occurs immediately after S2 Why? Resistance to filling of ventricles note: also called a ventricular gallop * it a caused by overload * use diaphraghm ( it is a high sound)
�cont. EXTRA HEART SOUNDS
S4 This occurs at the end of diastole, just before the next S1 Why? The Atrium contract & push blood into a non-compliant ventricles. NOTE: also called an atrial gallop * caused by hypertension, Aortic stenosis, cardiompathy * used bell to listen as it is a low sound
�GRADING OF MURMURS
Use VI point grading scale & record as fraction (ie. l/ lV or ll/Vl )
Grades: GRADE I : barely audible w/ stethoscope, often considered physiologic not pathologic. Requires concentration and quiet environment GRADE II: Very soft but distinctly audible GRADE III: moderately loud: there is no thrill or thrusting motion associated w/ the murmur GRADE IV: distinctly loud in addition to a palpable thrill GRADE V: very loud can actually hear w/ part of the diaphragm of the stethoscope off the chest palpable thrustand thrill present
�MURMURS
Caused by turbulence
Therefore we hear a gentle blowing, harsh,musical,raspy and rumbing sound
Why?
1.Velocity of blood increases (eg. Exercise)
2. Velocity of blood decreases (eg. Anemia) 3. Structural defect in valves or unsual opening accurs in chambers
�Classifications of heart murmurs sound
AORTIC STENOSIS Usually harsh, coarse Pitch: medium Radiation: most commonly neck into carotid area and down left sternal border,possibly apex
�Cont. Classifications of heart murmurs sound
PULMONARY STENOSIS Usually harsh Pitch: medium Radiation: toward the left upper neck and shoulder areas
�Cont. Classifications of heart murmurs sound
MITRAL REGURTATION Blowing and can be harsh in sound quality Pitch: high Radiation: usually to left axilla, LSB and base
�Cont. Classifications of heart murmurs sound
TRICUSPID REGURGITATION Blowing PITCH: high RADIATION: May radiate to LSB and MCL but not to axilla
� TRICUSPID STENOSIS Rumbling PITCH: low RADIATION: rare
MITRAL STENOSIS Rumbling PITCH: low and best heard with bell RADIATION: rare
�panocardiograms from normal and abnormal heart sounds
�Electrocardiogram
A normal ECG (top) indicates that the heart is functioning properly. The P wave occurs just prior to atrial contraction; the QRS complex occurs just prior to ventricular contraction; and the T wave occurs when the ventricles are recovering from contraction. Ventricular fibrillation (bottom) produces an irregular electrocardiogram due to irregular stimulation of the ventricles. Ventricular fibrillation is of special interest because it can be caused by an injury or drug overdose. It is the most common cause of sudden cardiac death in a seemingly healthy person over age 35. Once the ventricles are fibrillating, they have to be defibrillated by applying a strong electrical current for a short period of time. Then the SA node may be able to reestablish a coordinated beat.
�Thank you for listening! ^-^