You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- ECG InterpretationDocument81 pagesECG InterpretationaldiansyahraufNo ratings yet
- In The Name of God: Cardiogenic Pulmonary EdemaDocument51 pagesIn The Name of God: Cardiogenic Pulmonary EdemaaldiansyahraufNo ratings yet
- Absorpsi Makromolekuler Oleh Usus Atan Baas Sinuhaji Bika Fk-Usu/Rs HamDocument22 pagesAbsorpsi Makromolekuler Oleh Usus Atan Baas Sinuhaji Bika Fk-Usu/Rs HamaldiansyahraufNo ratings yet
- Fever in Children and FUODocument61 pagesFever in Children and FUOaldiansyahraufNo ratings yet
- Appendix 5. Melbourne Ambulance Stroke Screen (MASS) : Clinical History ElementsDocument1 pageAppendix 5. Melbourne Ambulance Stroke Screen (MASS) : Clinical History ElementsaldiansyahraufNo ratings yet
- Hyponatremia in Neurological Diseases in ICU: Review ArticleDocument5 pagesHyponatremia in Neurological Diseases in ICU: Review ArticlealdiansyahraufNo ratings yet
- Best Practice & Research Clinical Endocrinology & MetabolismDocument9 pagesBest Practice & Research Clinical Endocrinology & MetabolismaldiansyahraufNo ratings yet
- Lampiran: GMBR B. (1) Furunkel, (2) Karbunkel GMBR B. (1) Furunkel, (2) Karbunkel GMBR A. Folikulitis GMBR A. FolikulitisDocument4 pagesLampiran: GMBR B. (1) Furunkel, (2) Karbunkel GMBR B. (1) Furunkel, (2) Karbunkel GMBR A. Folikulitis GMBR A. FolikulitisaldiansyahraufNo ratings yet
- Tugas Dr. ATJSDocument7 pagesTugas Dr. ATJSaldiansyahraufNo ratings yet
- Sabiston Textbook of Surgery, 19th Ed: VGHTCDocument85 pagesSabiston Textbook of Surgery, 19th Ed: VGHTCaldiansyahraufNo ratings yet
- Lymphangitis & LymphadenitisDocument6 pagesLymphangitis & LymphadenitisaldiansyahraufNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
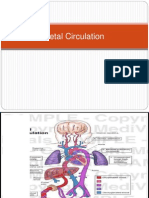
- Fetal CirculationDocument13 pagesFetal CirculationPraveen YadavNo ratings yet
- HUMAN ANATOMY AND PHYSIOLOGY LABORATORY Cardiovascular SystemDocument12 pagesHUMAN ANATOMY AND PHYSIOLOGY LABORATORY Cardiovascular SystemZaira MangalimanNo ratings yet
- 1.conginital Cardiac DefectsDocument39 pages1.conginital Cardiac DefectsJõsëph Jåy MîthNo ratings yet
- Fetal CirculationDocument10 pagesFetal CirculationprembarnabasNo ratings yet
- Introduction To The CvsDocument43 pagesIntroduction To The CvsParmesh PandeyNo ratings yet
- Fetal CirculationDocument28 pagesFetal CirculationNelai GoNo ratings yet
- Ob Evaluation 1 Final - Sec ADocument33 pagesOb Evaluation 1 Final - Sec AKarla Mae Israel CamarintaNo ratings yet
- Obladen 2010Document7 pagesObladen 2010Barna ÉvaNo ratings yet
- Ana&Physio of CV SystemDocument4 pagesAna&Physio of CV SystemNadia Andrea Paz AmoraNo ratings yet
- Foetal CirculationDocument8 pagesFoetal CirculationMujahid_Dean_8976No ratings yet
- 12 - Semiotics of Cardiovascular Disorders. Semiotics of Congenital Hert Diseases in Children.Document30 pages12 - Semiotics of Cardiovascular Disorders. Semiotics of Congenital Hert Diseases in Children.Omowunmi KadriNo ratings yet
- Abo Case Final Study-LatestDocument56 pagesAbo Case Final Study-LatestJonathan DiazNo ratings yet
- CHD ModuleDocument204 pagesCHD ModuleKellie RollinsNo ratings yet
- Update Fetal Circulation - MDM AmyDocument10 pagesUpdate Fetal Circulation - MDM AmyNana Yunus100% (1)
- Core Topics in Congenital Cardiac SurgeryDocument148 pagesCore Topics in Congenital Cardiac SurgeryLyse lilyNo ratings yet
- Pediatric CardiologyDocument7 pagesPediatric CardiologyMaikka IlaganNo ratings yet
- Physiologic Transition From Intrauterine To Extrauterine LifeDocument6 pagesPhysiologic Transition From Intrauterine To Extrauterine LifeGina M. TañedoNo ratings yet
- CASE-PRESENTATION-Bronchopulmonary DysplasiaDocument112 pagesCASE-PRESENTATION-Bronchopulmonary DysplasiaLouie MansaNo ratings yet
- Fetal Circulation ORIGINALDocument13 pagesFetal Circulation ORIGINALombir007No ratings yet
- 3 - Nursing Role in Reproductive and Sexual HealthDocument10 pages3 - Nursing Role in Reproductive and Sexual HealthShanealle Athaliah Magsalay CuaNo ratings yet
- In The Fetal CirculationDocument1 pageIn The Fetal CirculationJesena SalveNo ratings yet
- IMD - Step-Up To USMLE Step 3 - Chapter 1 - CardiologyDocument124 pagesIMD - Step-Up To USMLE Step 3 - Chapter 1 - CardiologyAly SherifNo ratings yet
- SCGS 2020 Biology Prelim P2 - MSDocument22 pagesSCGS 2020 Biology Prelim P2 - MSAnshul Bhangale100% (1)
- Maternal & Child Nursing Achievement Test FIRST SEMESTER 2021-2022Document13 pagesMaternal & Child Nursing Achievement Test FIRST SEMESTER 2021-2022Matelyn Oarga100% (1)
- 4 EL Husseinys Essentials of Cardiovascular System @eduwaves360Document236 pages4 EL Husseinys Essentials of Cardiovascular System @eduwaves360ahmed_abu_alrobNo ratings yet
- Fetal Circulation (For MBBS)Document50 pagesFetal Circulation (For MBBS)Tashif100% (1)
- Maternity Nursing An Introductory Text 11th Edition Leifer Test BankDocument9 pagesMaternity Nursing An Introductory Text 11th Edition Leifer Test BankSerenaNo ratings yet
- Normal PregnancyDocument65 pagesNormal PregnancyRhesie Joyce AguilarNo ratings yet
- Newborn Physiology PathologyDocument99 pagesNewborn Physiology Pathologythev0206100% (1)
- Fertilization To Conception: Maternal and Child Health Nursing PregnancyDocument8 pagesFertilization To Conception: Maternal and Child Health Nursing PregnancyNikki M. Arapol100% (1)