You might also like
- 2 PPT - CH - 03 Copy Decision MakingDocument30 pages2 PPT - CH - 03 Copy Decision MakingSultan SalmanNo ratings yet
- Hinkle PPT CH 28Document34 pagesHinkle PPT CH 28Ahmed AbahraNo ratings yet
- Concepts and Theories of Aging: Princy Francis M I Yr MSC (N) JmconDocument48 pagesConcepts and Theories of Aging: Princy Francis M I Yr MSC (N) Jmconcj bariasNo ratings yet
- Assessment and Management of Patients With Vascular Disorders and Problems of Peripheral CirculationDocument45 pagesAssessment and Management of Patients With Vascular Disorders and Problems of Peripheral CirculationCarlos RiosNo ratings yet
- N100 Rle Back MassageDocument24 pagesN100 Rle Back MassagerlinaoNo ratings yet
- Chapter 22 Upper Respiratory DisorderDocument171 pagesChapter 22 Upper Respiratory DisorderAnnette Aquino GuevarraNo ratings yet
- Chapter 05: Chronic Illness and Older Adults Harding: Lewis's Medical-Surgical Nursing, 11th EditionDocument8 pagesChapter 05: Chronic Illness and Older Adults Harding: Lewis's Medical-Surgical Nursing, 11th EditionTyler TappNo ratings yet
- NCM 0114 Module 4 Audio PowerpointDocument20 pagesNCM 0114 Module 4 Audio PowerpointKristine KimNo ratings yet
- Ii. Week 1 Module: Learning Content: Standards of Nursing PracticeDocument68 pagesIi. Week 1 Module: Learning Content: Standards of Nursing PracticeKaye bagasinNo ratings yet
- CM - Community Diagnosis - ParasDocument83 pagesCM - Community Diagnosis - ParasHoque Mohammed Newaz Shoriful100% (1)
- M1 - Nusing Care ManagementDocument40 pagesM1 - Nusing Care ManagementKristine KimNo ratings yet
- Week 9 - Ch. 31 - SkinDocument31 pagesWeek 9 - Ch. 31 - SkinMary SingletonNo ratings yet
- Funda RLE RD Time TableDocument4 pagesFunda RLE RD Time Tablemj CanilangNo ratings yet
- Chapter 003Document9 pagesChapter 003Erika MidkiffNo ratings yet
- Dementia Power PointDocument23 pagesDementia Power Pointapi-253856690No ratings yet
- Module IDocument34 pagesModule INelly CruzNo ratings yet
- Geria (Midterms)Document42 pagesGeria (Midterms)ANGELA GLORIA LAPUZNo ratings yet
- The Nursing Health History (NHH) : NCM 101-A: Health AssessmentDocument7 pagesThe Nursing Health History (NHH) : NCM 101-A: Health Assessmentthe someoneNo ratings yet
- Introduction To The Cardiovascular SystemDocument22 pagesIntroduction To The Cardiovascular Systemwaqas_xsNo ratings yet
- Gerontology LectureDocument70 pagesGerontology LectureAlessandra MercadoNo ratings yet
- Lesson 5 Core Elements Evidenced Based Gerontological Nursing PracticeDocument38 pagesLesson 5 Core Elements Evidenced Based Gerontological Nursing PracticeSam GarciaNo ratings yet
- Week 1 PPT Community ConceptsDocument48 pagesWeek 1 PPT Community ConceptsK DNo ratings yet
- Geria FinalsDocument14 pagesGeria FinalsAlliah RodriguezNo ratings yet
- Assessment of Cardiovascular FunctionDocument33 pagesAssessment of Cardiovascular FunctionBav VAansoqnuaetzNo ratings yet
- The Nursing ProcessDocument94 pagesThe Nursing Processmutlabans100% (1)
- Care of Older Adults (Prelims)Document12 pagesCare of Older Adults (Prelims)Ax’l SisterNo ratings yet
- Procedural Checklist NCM 112 RLE Preparing A Sterile Field Opening A Sterile Pack Adding Items To A Sterile Field Adding Liquids To A Sterile Field Skin PreparationDocument5 pagesProcedural Checklist NCM 112 RLE Preparing A Sterile Field Opening A Sterile Pack Adding Items To A Sterile Field Adding Liquids To A Sterile Field Skin PreparationAbegail Eliah EstalaneNo ratings yet
- Demographics of AgingDocument19 pagesDemographics of AgingAnalyn SarmientoNo ratings yet
- Older Patients Care RegimeDocument8 pagesOlder Patients Care RegimeMarie Ashley CasiaNo ratings yet
- NCM 114 Module 1Document7 pagesNCM 114 Module 1Roel John Atamosa CasilacNo ratings yet
- Geria UNIT 3Document5 pagesGeria UNIT 3Raiden VizcondeNo ratings yet
- File 9Document43 pagesFile 9Johanine VillasantiagoNo ratings yet
- NCM 114 ReviewerDocument9 pagesNCM 114 ReviewerLovely DaroleNo ratings yet
- NCM101 Collection of Objective Data (Validation of Data)Document50 pagesNCM101 Collection of Objective Data (Validation of Data)Roland100% (1)
- Perception & Coordination NCM 104Document162 pagesPerception & Coordination NCM 104bianqueeNo ratings yet
- MODULE NCM 114 Module 6 3 1 1Document6 pagesMODULE NCM 114 Module 6 3 1 1Keesha Mae Urgelles TimogNo ratings yet
- Hinkle PPT CH 18Document20 pagesHinkle PPT CH 18maniz442100% (1)
- 1 Gerontology Nursing Concepts: Gloria P. de Leon, RN, RM, ManDocument211 pages1 Gerontology Nursing Concepts: Gloria P. de Leon, RN, RM, ManJohanine VillasantiagoNo ratings yet
- 3 Family Nursing Care ProcessDocument22 pages3 Family Nursing Care ProcessKenn NuydaNo ratings yet
- Skin - Hair.Nails Head & Neck Eyes. Ears. Nose. Sinuses Mouth. PharynxDocument92 pagesSkin - Hair.Nails Head & Neck Eyes. Ears. Nose. Sinuses Mouth. PharynxAT4-11 HUMSS 2 CEDRICK ILAO100% (1)
- Unit 1: Concepts, Principles, and Theories in The Care of Older AdultsDocument10 pagesUnit 1: Concepts, Principles, and Theories in The Care of Older AdultsEricson CandelariaNo ratings yet
- Nursing ProcessDocument8 pagesNursing ProcessGhadeer Hijazeen100% (1)
- Childhood and Adolescent DisorderDocument54 pagesChildhood and Adolescent DisorderRiccyNo ratings yet
- PWU NCM 114 - Care of The Older Person 3Document34 pagesPWU NCM 114 - Care of The Older Person 3Ira AnuddinNo ratings yet
- WEEK 1 CU1 History of Health EducationDocument5 pagesWEEK 1 CU1 History of Health EducationDaichi100% (1)
- Group 3 - CHN-CPDocument84 pagesGroup 3 - CHN-CPFan XiaoNo ratings yet
- NCM 103 SyllabusDocument10 pagesNCM 103 SyllabuslouradelNo ratings yet
- Maternal & Child Nursing Care: Lecture NotesDocument42 pagesMaternal & Child Nursing Care: Lecture NotesMidori San100% (1)
- Functional Health Patterns TABLEDocument3 pagesFunctional Health Patterns TABLEMelaNo ratings yet
- Care of The Older AdultDocument56 pagesCare of The Older AdultKarlon Moses Delfin PiniliNo ratings yet
- Gloving ChecklistDocument2 pagesGloving ChecklistlemuelNo ratings yet
- Historical Backgaround of Health EducationDocument12 pagesHistorical Backgaround of Health EducationDaichi100% (1)
- 1 COMMUNITY HEALTH NURSING CONCEPTS AutosavedDocument65 pages1 COMMUNITY HEALTH NURSING CONCEPTS AutosavedAbdhanie PanontonganNo ratings yet
- Community Health Assessment Tools: Week 7Document16 pagesCommunity Health Assessment Tools: Week 7ANGELICA MACASONo ratings yet
- Assignment in NCM 114Document1 pageAssignment in NCM 114camile buhanginNo ratings yet
- Chrinically Ill & Older Persons SyllabusDocument5 pagesChrinically Ill & Older Persons Syllabuskamae_27No ratings yet
- Family Health AssessmentDocument23 pagesFamily Health AssessmentPatrick Poculan100% (1)
- Pregnancy at Risk: Conditions That Complicate PregnancyDocument40 pagesPregnancy at Risk: Conditions That Complicate PregnancyHannaNo ratings yet
- Emergency NursingDocument40 pagesEmergency NursingEstherThompson100% (7)
- Chapter 034Document19 pagesChapter 034Mahmmoud FuqahaNo ratings yet
- AUSTRALIA Nursing and Midwifery Board Template Instructions To Accreditation AuthoritiesDocument2 pagesAUSTRALIA Nursing and Midwifery Board Template Instructions To Accreditation AuthoritiesPearl DiBerardinoNo ratings yet
- Salwa Maghrabi Teacher Assistant Nursing Department: Prepared byDocument30 pagesSalwa Maghrabi Teacher Assistant Nursing Department: Prepared byPearl DiBerardino100% (1)
- Novice To Expert P BennerDocument1 pageNovice To Expert P BennerMagilas S. SalvacionNo ratings yet
- Eruptive Fever DiseaseDocument61 pagesEruptive Fever DiseasePearl DiBerardino100% (2)
- Atrial Septal DefectDocument2 pagesAtrial Septal DefectPearl DiBerardinoNo ratings yet
- Airway SuctioningDocument30 pagesAirway SuctioningPearl DiBerardinoNo ratings yet
- Tracheostomy Suctioning ProcedureDocument1 pageTracheostomy Suctioning ProcedurePearl DiBerardinoNo ratings yet
- Chapter 17 End-Of-Life CareDocument29 pagesChapter 17 End-Of-Life CarePearl DiBerardinoNo ratings yet
- Evaluation Checklist For Nursing AideDocument2 pagesEvaluation Checklist For Nursing AidePearl DiBerardinoNo ratings yet
- Professional Communication in NursingDocument100 pagesProfessional Communication in NursingPearl DiBerardino100% (2)
- Case StudiesDocument17 pagesCase StudiesDamian Maguire100% (4)
- Parenting NLP 4 Kids 33 161Document2 pagesParenting NLP 4 Kids 33 161Mus Oub100% (1)
- Daftar Obat High AlertDocument31 pagesDaftar Obat High Alertmuin ritongaNo ratings yet
- Understanding POTS - The Invisible IllnessDocument10 pagesUnderstanding POTS - The Invisible IllnessSpencer100% (1)
- Career Interest Profiler ReflectionDocument2 pagesCareer Interest Profiler Reflectionapi-478464529No ratings yet
- North of Tyne Formulary Version 5 4finalDocument194 pagesNorth of Tyne Formulary Version 5 4finalAnonymous VfSIDMyrmENo ratings yet
- Untitled Document - Docx.1Document10 pagesUntitled Document - Docx.1Syeda Sabahat BatoolNo ratings yet
- Guidance ServicesDocument7 pagesGuidance ServicesJosephine Princess Ibanez SantosNo ratings yet
- Bereavement: Coping With A DeathDocument28 pagesBereavement: Coping With A DeathTheresa SuleNo ratings yet
- Decreased Intracranial Pressure With Optimal Head Elevation of 30 or 45 Degrees in Traumatic Brain Injury Patients (Literatur Review)Document4 pagesDecreased Intracranial Pressure With Optimal Head Elevation of 30 or 45 Degrees in Traumatic Brain Injury Patients (Literatur Review)Theresia Avila KurniaNo ratings yet
- Mental Health Nursing and First Episode Psychosis (2011 Dusseldorp)Document19 pagesMental Health Nursing and First Episode Psychosis (2011 Dusseldorp)Eric KatškovskiNo ratings yet
- Price Controls and EntryDocument33 pagesPrice Controls and EntryplatinumadNo ratings yet
- Beginner To Intermediate Yoga-DYWMDocument6 pagesBeginner To Intermediate Yoga-DYWMGeraldine QuintanaNo ratings yet
- Ever Increasing Faith Magazine - Issue 3 - 2013Document32 pagesEver Increasing Faith Magazine - Issue 3 - 2013jsuccessNo ratings yet
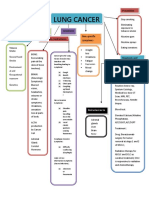
- Concept Map LungDocument1 pageConcept Map LungThea Eya FayeNo ratings yet
- Polypharmacy in Elderly PatientsDocument7 pagesPolypharmacy in Elderly PatientsMariana RibeiroNo ratings yet
- NCP For Acute Lymphocytic LeukemiaDocument7 pagesNCP For Acute Lymphocytic LeukemiaLilian Linogao100% (10)
- Myasthenia Gravis Anesthetic Implications and ManagementDocument31 pagesMyasthenia Gravis Anesthetic Implications and Managementaashish45No ratings yet
- Sr. No. Cghs Treatment Procedure/Investigation List Non-NABH/Non - NABL Rates Nabh/Nabl RatesDocument41 pagesSr. No. Cghs Treatment Procedure/Investigation List Non-NABH/Non - NABL Rates Nabh/Nabl RatesNarayanan NMNo ratings yet
- Prison Architecture and DesignDocument46 pagesPrison Architecture and Designbryant neutron100% (1)
- Ateneo de Zamboanga University: College of Nursing Nursing Skills Output (Nso) Week Biopsy I. DescritptionDocument4 pagesAteneo de Zamboanga University: College of Nursing Nursing Skills Output (Nso) Week Biopsy I. DescritptionHaifi HunNo ratings yet
- Calf Protocols Ver4Document6 pagesCalf Protocols Ver4Sadam Irshad100% (1)
- Eye DisordersDocument4 pagesEye DisordersJade SamonteNo ratings yet
- Psychiatric 12Document33 pagesPsychiatric 12Res TyNo ratings yet
- Food Cures For Spleen Qi Deficiency - Chinese MedicineDocument9 pagesFood Cures For Spleen Qi Deficiency - Chinese MedicineJ.J.No ratings yet
- Fatality Inquiry Report: Jeffrey & Jeremy BostickDocument54 pagesFatality Inquiry Report: Jeffrey & Jeremy BostickEmily MertzNo ratings yet
- Chapter 20 - Transitions TheoryDocument18 pagesChapter 20 - Transitions Theoryslb_21100% (3)
- Ciprofloxacin Induced Systemic Lupus ErythematosusDocument8 pagesCiprofloxacin Induced Systemic Lupus ErythematosusAvelox FloxNo ratings yet
- Fibroids PresentationDocument6 pagesFibroids Presentationapi-237061134No ratings yet
- Fluid and Electrolyte Therapy, Calculation of Fluids and Its AdministrationDocument11 pagesFluid and Electrolyte Therapy, Calculation of Fluids and Its AdministrationAnusha Verghese100% (2)