You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Superficial MycosisDocument17 pagesSuperficial Mycosisapi-19969058100% (2)
- Introduction To MycologyDocument18 pagesIntroduction To Mycologyapi-19969058100% (1)
- Opportunistic MycosisDocument19 pagesOpportunistic Mycosisapi-19969058No ratings yet
- Systemic MycosisDocument15 pagesSystemic Mycosisapi-19969058No ratings yet
- Immunity To ParasiteDocument8 pagesImmunity To Parasiteapi-19969058No ratings yet
- Echinococcus GranulosusDocument15 pagesEchinococcus Granulosusapi-19969058No ratings yet
- Filariasis: Dr. Mejbah Uddin AhmedDocument19 pagesFilariasis: Dr. Mejbah Uddin Ahmedapi-19969058No ratings yet
- Diagnosis of Viral DiseaseDocument20 pagesDiagnosis of Viral Diseaseapi-19969058No ratings yet
- H. NanaDocument2 pagesH. Nanaapi-19969058No ratings yet
- Paramyxovirus LecDocument25 pagesParamyxovirus Lecapi-19969058No ratings yet
- Discovery of Influenza Virus: - First Isolated From A Pig in 1931 (Swine Flu) - Isolated From Human in 1933Document16 pagesDiscovery of Influenza Virus: - First Isolated From A Pig in 1931 (Swine Flu) - Isolated From Human in 1933api-19969058No ratings yet
- Human Immunodeficiency Virus LectureDocument34 pagesHuman Immunodeficiency Virus Lectureapi-19969058No ratings yet
- Herpes Viruses LectureDocument46 pagesHerpes Viruses Lectureapi-19969058100% (1)
- Poxvirus: Family Includes: Smallpox Virus (Variola Virus) Vaccinia Virus Molluscum Contagiosum VirusDocument19 pagesPoxvirus: Family Includes: Smallpox Virus (Variola Virus) Vaccinia Virus Molluscum Contagiosum Virusapi-19969058No ratings yet
- Antiviral Drugs: Dr. Mejbah Uddin AhmedDocument10 pagesAntiviral Drugs: Dr. Mejbah Uddin Ahmedapi-19969058No ratings yet
- Autoimmunity and ToleranceDocument17 pagesAutoimmunity and Toleranceapi-19969058No ratings yet
- Acquired Immunity: Dr. Mejbah Uddin AhmedDocument13 pagesAcquired Immunity: Dr. Mejbah Uddin Ahmedapi-19969058No ratings yet
- Immunoprophylaxis and Immunotherapy: Dr. Mejbah Uddin AhmedDocument19 pagesImmunoprophylaxis and Immunotherapy: Dr. Mejbah Uddin Ahmedapi-19969058No ratings yet
- Diagnostic Techniques in BacteriologyDocument17 pagesDiagnostic Techniques in Bacteriologyapi-19969058No ratings yet
- Immunodef Iciency: Dr. Mejbah Uddin AhmedDocument16 pagesImmunodef Iciency: Dr. Mejbah Uddin Ahmedapi-19969058No ratings yet
- Bacterial PathogenesisDocument36 pagesBacterial Pathogenesisapi-19969058100% (3)
- Bacteriological Culture MediaDocument18 pagesBacteriological Culture Mediaapi-19969058No ratings yet
- Tumor Immunity: DR. Mejbah Uddin AhmedDocument21 pagesTumor Immunity: DR. Mejbah Uddin Ahmedapi-19969058No ratings yet
- Serratia MarcescensDocument20 pagesSerratia Marcescenstummalapalli venkateswara raoNo ratings yet
- HepatomaDocument5 pagesHepatomaJose Emmanuel FranciaNo ratings yet
- Lecture of Zoonoses at NTU 2015Document159 pagesLecture of Zoonoses at NTU 2015polypeptideNo ratings yet
- Blood and Tissue Nematodes in Man PDFDocument7 pagesBlood and Tissue Nematodes in Man PDFRizzy VillanuevaNo ratings yet
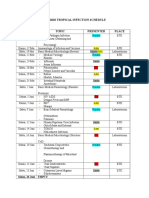
- Imo Tropical Infection ScheduleDocument3 pagesImo Tropical Infection ScheduleHendroMaleNo ratings yet
- Biology Class 12 ProjectDocument26 pagesBiology Class 12 ProjectZinzekoNo ratings yet
- Standard Operating Process and Rules Joining The Campus: Bits Pilani, K K Birla Goa CampusDocument2 pagesStandard Operating Process and Rules Joining The Campus: Bits Pilani, K K Birla Goa CampusPrit PethaniNo ratings yet
- 20 Besar Penyakit 23Document18 pages20 Besar Penyakit 23SudiroeNo ratings yet
- Pendekatan Desain Dan Aplikasi Ruang Praktek Dokter Gigi Di Masa PandemiDocument13 pagesPendekatan Desain Dan Aplikasi Ruang Praktek Dokter Gigi Di Masa PandemiKeyla Maharani AddlewishNo ratings yet
- Hubungan Dukungan Keluarga Dengan Kepatuhan Minum Obat Pada Penderita TB Paru Di Puskesmaspadang Bulan MedanDocument7 pagesHubungan Dukungan Keluarga Dengan Kepatuhan Minum Obat Pada Penderita TB Paru Di Puskesmaspadang Bulan MedanSiti KomariahNo ratings yet
- WHOnet Preparation and Antibiogram InterpretationDocument2 pagesWHOnet Preparation and Antibiogram Interpretationarmada thamNo ratings yet
- Occupational Health (Health Screening Questionnaire)Document6 pagesOccupational Health (Health Screening Questionnaire)earl-e-birdNo ratings yet
- Sahya Part 1Document69 pagesSahya Part 1Homeopathy Torrents100% (2)
- Mr. Abhishek J DanesDocument2 pagesMr. Abhishek J DanesAbhishek DanesNo ratings yet
- Caso Clínico 6Document5 pagesCaso Clínico 6Rodrigo Jesús Alejandro Abanto SánchezNo ratings yet
- Diseases Caused by PathogensDocument2 pagesDiseases Caused by PathogensbrajanosmaniNo ratings yet
- 4a Rota-Vaccine Administration KenyaDocument21 pages4a Rota-Vaccine Administration KenyaSandraNo ratings yet
- Urinary Tract InfectionsDocument3 pagesUrinary Tract InfectionsBimbi ZulkifliNo ratings yet
- SLMC Health Declaration FormDocument1 pageSLMC Health Declaration FormNikkiNo ratings yet
- Micro Bacteriology PDFDocument4 pagesMicro Bacteriology PDFMasroor ShahNo ratings yet
- 2012 Number 1 947445146213461Document5 pages2012 Number 1 947445146213461MedstudNo ratings yet
- Scabies Treatment ProphylaxisDocument4 pagesScabies Treatment Prophylaxisduch2020No ratings yet
- A. Cotton Blue: False TrueDocument5 pagesA. Cotton Blue: False TrueDevinViscars100% (1)
- Scrub TyphusDocument4 pagesScrub TyphusVijaya Aditya TadepalliNo ratings yet
- MA COVID-19 Checklist: Office SpacesDocument2 pagesMA COVID-19 Checklist: Office Spacessafira dwiajengNo ratings yet
- Mites and LiceDocument2 pagesMites and LiceJohn OneillNo ratings yet
- KundiDocument10 pagesKundirio1995No ratings yet
- ClinicalStagesofHIVBiolixir Published2011Document4 pagesClinicalStagesofHIVBiolixir Published2011Lyzia AushaNo ratings yet
- Nur SuciyantiDocument8 pagesNur SuciyantiRabi'a KadirNo ratings yet
- Kti Selly Alvionita TanjungDocument57 pagesKti Selly Alvionita TanjungDini MardhiyaniNo ratings yet