You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Keynote Intermediate Test 1Document5 pagesKeynote Intermediate Test 1peienglish33% (3)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Temple of The Etherians (Scrolls of Illumination)Document91 pagesTemple of The Etherians (Scrolls of Illumination)Δαμοκλῆς Στέφανος81% (16)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Critical ThinkingDocument6 pagesCritical ThinkingmatrixtrinityNo ratings yet
- Intelligence in PsychologyDocument29 pagesIntelligence in PsychologymatrixtrinityNo ratings yet
- Stress and Illness: Castillo, Justine GDocument19 pagesStress and Illness: Castillo, Justine GmatrixtrinityNo ratings yet
- Group Number: Case Title: Year and Section: Group Members: 1. 5. 2. 6. 3. 7. 4. 8Document1 pageGroup Number: Case Title: Year and Section: Group Members: 1. 5. 2. 6. 3. 7. 4. 8matrixtrinityNo ratings yet
- antepartumTEST1 MOSBYDocument14 pagesantepartumTEST1 MOSBYmatrixtrinity50% (2)
- Antepartumtest2 LippincottDocument7 pagesAntepartumtest2 Lippincottmatrixtrinity100% (1)
- Distinguishing Features of Anthropology - Characteristics 1-5 6.78 What Are The3 Unique Approaches of AnthropologyDocument2 pagesDistinguishing Features of Anthropology - Characteristics 1-5 6.78 What Are The3 Unique Approaches of AnthropologymatrixtrinityNo ratings yet
- Intestinal Obstruction5Document4 pagesIntestinal Obstruction5matrixtrinityNo ratings yet
- Socio - GENDER, ETHNICITY AND RACEDocument22 pagesSocio - GENDER, ETHNICITY AND RACEmatrixtrinity100% (1)
- Cardio DiseasesDocument17 pagesCardio DiseasesmatrixtrinityNo ratings yet
- Intestinal Obstruction Wit Pic2Document2 pagesIntestinal Obstruction Wit Pic2matrixtrinityNo ratings yet
- Blood ComponentDocument33 pagesBlood Componentmatrixtrinity100% (1)
- Cardiovascular Physio Logic ProcessDocument35 pagesCardiovascular Physio Logic ProcessmatrixtrinityNo ratings yet
- What Is Intestinal ObstructionDocument5 pagesWhat Is Intestinal ObstructionmatrixtrinityNo ratings yet
- Cerebrovascular Accidents: Rochee P. Benito, RNDocument23 pagesCerebrovascular Accidents: Rochee P. Benito, RNmatrixtrinityNo ratings yet
- Circulatory System: Rochi Paraon Benito, RN Infection Control NurseDocument15 pagesCirculatory System: Rochi Paraon Benito, RN Infection Control NursematrixtrinityNo ratings yet
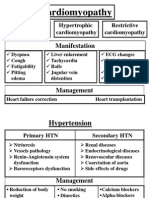
- Cardiomyopathy 02Document2 pagesCardiomyopathy 02matrixtrinityNo ratings yet
- Cardiovascular Therapeutic ManagementDocument15 pagesCardiovascular Therapeutic ManagementmatrixtrinityNo ratings yet
- Burns and Environmental EmergenciesDocument33 pagesBurns and Environmental EmergenciesmatrixtrinityNo ratings yet
- BDJOBS AssignmentDocument4 pagesBDJOBS AssignmentMurshid IqbalNo ratings yet
- A - Nahm27,+581 1746 4 EDDocument10 pagesA - Nahm27,+581 1746 4 EDistiqamahNo ratings yet
- 2019 CPDDocument61 pages2019 CPDSalleurNo ratings yet
- Siomai Ni DiegoDocument21 pagesSiomai Ni DiegoKimberly Lagman82% (17)
- Icd 10 CodeDocument9 pagesIcd 10 CodeFloriPuspaHumaniNo ratings yet
- Horns & Fanfares BrochureDocument20 pagesHorns & Fanfares BrochureGowthamNo ratings yet
- CENTERLINE 2100 Motor Control Centers: Selection GuideDocument62 pagesCENTERLINE 2100 Motor Control Centers: Selection GuideLeonel CarbonettiNo ratings yet
- Breasts in The Age of NapoleonDocument12 pagesBreasts in The Age of NapoleonTeodor BurnarNo ratings yet
- New Revised Franchisee Business Prop (1) .Document6 pagesNew Revised Franchisee Business Prop (1) .bindasgoyalNo ratings yet
- Conceptualisation of Gender Based Violence in ZimbabweDocument10 pagesConceptualisation of Gender Based Violence in ZimbabweRed KnightNo ratings yet
- Essay 1Document1 pageEssay 1David AkinlamiNo ratings yet
- Preparation of Cholesteryl Ester Liquid CrystalsDocument11 pagesPreparation of Cholesteryl Ester Liquid Crystalsuttamkumar_mondol_5No ratings yet
- 3SI - MOP Proposal Face Mask-Min PDFDocument22 pages3SI - MOP Proposal Face Mask-Min PDFverawati100% (1)
- Mammo1012C enDocument2 pagesMammo1012C enLizzy DuronNo ratings yet
- LA Diocese Abuse Report 2004 (Part 2)Document155 pagesLA Diocese Abuse Report 2004 (Part 2)Justin BobbyNo ratings yet
- Case Presentation DVTDocument26 pagesCase Presentation DVTimad mokalledNo ratings yet
- Group 19Document24 pagesGroup 19abhishek kumarNo ratings yet
- Technical Service Report TemplateDocument4 pagesTechnical Service Report TemplateKamarulAnuar TarmiziNo ratings yet
- Waste Incineration Insert v2Document2 pagesWaste Incineration Insert v2Namik HadziibrahimovicNo ratings yet
- Final BPDocument39 pagesFinal BPapi-19471040No ratings yet
- Odb CdiDocument644 pagesOdb CdiPaul JagdharryNo ratings yet
- Salaries & Wages - Regular Payroll PERA . Due To BIRDocument7 pagesSalaries & Wages - Regular Payroll PERA . Due To BIRAyie RomeroNo ratings yet
- Food Product Recall ProcedureDocument11 pagesFood Product Recall Procedureadhe hildaNo ratings yet
- Exp 2 Dry FractionationDocument10 pagesExp 2 Dry Fractionationtusen krishNo ratings yet
- Purchase - Specification - For PAC Dosing - AgitatorDocument2 pagesPurchase - Specification - For PAC Dosing - Agitatorcontactdevansh1174No ratings yet
- Author's Accepted Manuscript: Journal of Affective DisordersDocument3 pagesAuthor's Accepted Manuscript: Journal of Affective DisordersEzekiel LucasNo ratings yet
- FLS ValveDocument2 pagesFLS Valvegamalyehia13100% (1)
- DaburDocument27 pagesDaburKeshav KalaniNo ratings yet