You might also like
- History Taking in OrthopaedicsDocument23 pagesHistory Taking in OrthopaedicsVaibhav Krishna100% (5)
- Neonatal JaundiceDocument33 pagesNeonatal JaundiceVaibhav Krishna100% (2)
- 2012 Fall TSJ s03 The Mystery of The Gospel PT 1 - Stuart GreavesDocument5 pages2012 Fall TSJ s03 The Mystery of The Gospel PT 1 - Stuart Greavesapi-164301844No ratings yet
- TH LeukemiaDocument8 pagesTH Leukemiaأحمد علي حبيبNo ratings yet
- Chronic Myeloid Leukemia (CML) - Hematology and Oncology - MSD Manual Professional EditionDocument3 pagesChronic Myeloid Leukemia (CML) - Hematology and Oncology - MSD Manual Professional Editionnurul auliaNo ratings yet
- Acute Lymphoblastic LeukemiaDocument34 pagesAcute Lymphoblastic LeukemiamtyboyNo ratings yet
- Acute LeukemiaDocument6 pagesAcute LeukemiaYolanda UriolNo ratings yet
- Acute Myeloid LuekemiaDocument30 pagesAcute Myeloid LuekemiaKathleen DimacaliNo ratings yet
- Chronic LeukemiaDocument12 pagesChronic LeukemiaJuan RamirezNo ratings yet
- Background: Pediatric Acute Lymphoblastic LeukemiaDocument3 pagesBackground: Pediatric Acute Lymphoblastic LeukemiaNitin KumarNo ratings yet
- Ojim 2016091213324550Document10 pagesOjim 2016091213324550rianmg21No ratings yet
- Chronic Myeloid LeukaemiaDocument30 pagesChronic Myeloid Leukaemiajismi vallachiraNo ratings yet
- All Aml NCCN 2023 HamidahDocument45 pagesAll Aml NCCN 2023 HamidahPPDS IPD ULMNo ratings yet
- From The Experts: How I Treat Older Patients With Acute Myeloid LeukemiaDocument12 pagesFrom The Experts: How I Treat Older Patients With Acute Myeloid LeukemiaWillyPeñaNo ratings yet
- Chronic Lymphocytic Leukemia (CLL)Document17 pagesChronic Lymphocytic Leukemia (CLL)Lalie PalmaNo ratings yet
- Acute Lymphoblastic Leukemia: Differential DiagnosisDocument6 pagesAcute Lymphoblastic Leukemia: Differential DiagnosisIma OhwNo ratings yet
- Acute Leukemia ThesisDocument8 pagesAcute Leukemia Thesisafcnftqep100% (2)
- Pediatric LeukemiasDocument42 pagesPediatric LeukemiasFilbertaNo ratings yet
- Relapsed Refractory AMLDocument114 pagesRelapsed Refractory AMLKishoreChandraKoradaNo ratings yet
- Chronic Myeloid Leukemia HammadDocument33 pagesChronic Myeloid Leukemia HammadFaizan AhmedNo ratings yet
- Myeloid and Lymphoid MalignanciesDocument67 pagesMyeloid and Lymphoid MalignanciesAdit PrayogaNo ratings yet
- Hematopoietic Acute Radiation Syndrome (Aplastic Anemia, Bone Marrow Syndrome)Document32 pagesHematopoietic Acute Radiation Syndrome (Aplastic Anemia, Bone Marrow Syndrome)Dmitri PopovNo ratings yet
- Chronic Leukemia HerfindalDocument40 pagesChronic Leukemia HerfindalAanshi ShahNo ratings yet
- Prognosis and Therapy When Acute Promyelocytic Leukemia and Other "Good Risk" Acute Myeloid Leukemias Occur As A Therapy Myeloid NeoplasmDocument7 pagesPrognosis and Therapy When Acute Promyelocytic Leukemia and Other "Good Risk" Acute Myeloid Leukemias Occur As A Therapy Myeloid NeoplasmClinica MonserratNo ratings yet
- Leukemia and Nervous System PDFDocument25 pagesLeukemia and Nervous System PDFhawinnurdianaNo ratings yet
- Chronic Myeloid LeukemiaDocument37 pagesChronic Myeloid LeukemialoveNo ratings yet
- Bioe 326Document5 pagesBioe 326Farah TubasiNo ratings yet
- Acute Myeloid Leukemia SubtypesDocument5 pagesAcute Myeloid Leukemia SubtypesPeter Lucky TurianoNo ratings yet
- Myelodysplastic Syndromes: Jorge E. Cortes,, Alan List,, and Hagop KantarjianDocument16 pagesMyelodysplastic Syndromes: Jorge E. Cortes,, Alan List,, and Hagop KantarjianjarleneccNo ratings yet
- Hematologic Malignancies: SMF Hematologi-Onkologi Medik Ilmu Penyakit DalamDocument72 pagesHematologic Malignancies: SMF Hematologi-Onkologi Medik Ilmu Penyakit DalamAstri Arri FebriantiNo ratings yet
- The Role of Inflammation in Leukaemia: Janusz Krawczyk, Michael O'Dwyer, Ronan Swords, Ciara Freeman and Francis J GilesDocument26 pagesThe Role of Inflammation in Leukaemia: Janusz Krawczyk, Michael O'Dwyer, Ronan Swords, Ciara Freeman and Francis J GilesCandle Jo'inNo ratings yet
- Bone Marrow Failure and Severe Aplastic Anemia Revision 1.1Document3 pagesBone Marrow Failure and Severe Aplastic Anemia Revision 1.1Rasha Al MousaNo ratings yet
- LeukemiaDocument38 pagesLeukemiabikeyNo ratings yet
- Acute Myeloid Leukemia ThesisDocument5 pagesAcute Myeloid Leukemia ThesisBuyCheapEssayOmaha100% (2)
- Trombocytopenia in CaDocument7 pagesTrombocytopenia in CaanisaNo ratings yet
- Acute Leukaemias Lecture-1Document39 pagesAcute Leukaemias Lecture-1MarvellousNo ratings yet
- Am J Hematol 2022 MM UpdateDocument22 pagesAm J Hematol 2022 MM UpdateLu BattipiedeNo ratings yet
- Ahmad Sh. Silmi MSC Haematology, FIBMSDocument63 pagesAhmad Sh. Silmi MSC Haematology, FIBMSHadi AdamNo ratings yet
- Dipiro 8 Th-Halaman-2410-2446 PDFDocument37 pagesDipiro 8 Th-Halaman-2410-2446 PDFFarmasi 4No ratings yet
- Leukemia Thesis PDFDocument5 pagesLeukemia Thesis PDFjpwvbhiig100% (2)
- Leptomeningeal DiseaseDocument17 pagesLeptomeningeal DiseaseForem ZayneNo ratings yet
- Chronic Myeloid Leukemia: 2020 Update On Diagnosis, Therapy and MonitoringDocument19 pagesChronic Myeloid Leukemia: 2020 Update On Diagnosis, Therapy and MonitoringRiyadh Z. MawloodNo ratings yet
- Curroncol 29 00491Document15 pagesCurroncol 29 00491CT DAMNo ratings yet
- Acute Lymphoblastic Leukemia DR - Hussein AlatabiDocument21 pagesAcute Lymphoblastic Leukemia DR - Hussein AlatabiSaman SarKoNo ratings yet
- Chronic Myeloid Leukemia Dissertation ThesisDocument8 pagesChronic Myeloid Leukemia Dissertation ThesisHelpWithFilingDivorcePapersCanada100% (2)
- Cancers 12 01746 v2Document18 pagesCancers 12 01746 v2Ulicer CruzNo ratings yet
- Cancers 12 01746Document18 pagesCancers 12 01746LauraQuinteroNo ratings yet
- Case Study Leukemia ScribdDocument3 pagesCase Study Leukemia ScribdJhoiiceeNo ratings yet
- Kuliah Kelainan Leukosit & RES - ZIADocument114 pagesKuliah Kelainan Leukosit & RES - ZIAannnisaNo ratings yet
- Acute Myeloblastic Leukaemia: BY DR Halima Talba Consultant Haematologist Department of Haematology and BtsDocument44 pagesAcute Myeloblastic Leukaemia: BY DR Halima Talba Consultant Haematologist Department of Haematology and BtsMuhammad Modu BulamaNo ratings yet
- Clinical Manifestations, Pathologic Features, and Diagnosis of Acute Promyelocytic Leukemia in AdultsDocument10 pagesClinical Manifestations, Pathologic Features, and Diagnosis of Acute Promyelocytic Leukemia in AdultsANDREEA-CORNELIA NECULCEANo ratings yet
- Caso AuntmineDocument19 pagesCaso AuntmineJuan Manuel Chino MendozaNo ratings yet
- Leukemia in ChildrenDocument44 pagesLeukemia in ChildrenSami ShouraNo ratings yet
- Acute Leukemia Best ArticleDocument8 pagesAcute Leukemia Best ArticleMahesh T MadhavanNo ratings yet
- LLC 2006Document11 pagesLLC 2006claudia8a_ulamedNo ratings yet
- Acute Myeloid LeukemiaDocument15 pagesAcute Myeloid LeukemiaMedha DuttaNo ratings yet
- Acute Myeloid Leukemia A Concise ReviewDocument17 pagesAcute Myeloid Leukemia A Concise Reviewberlianza activiraNo ratings yet
- Renal CarcinomaDocument3 pagesRenal Carcinomalb25No ratings yet
- Thrombosis and Acute LeukemiaDocument6 pagesThrombosis and Acute Leukemiaannisa edwarNo ratings yet
- Acute Myeloid LeukemiaDocument11 pagesAcute Myeloid Leukemiafitra azraNo ratings yet
- Fast Facts: Measurable Residual Disease: A clearer picture for treatment decisionsFrom EverandFast Facts: Measurable Residual Disease: A clearer picture for treatment decisionsNo ratings yet
- Manipal College of Medical Sciences Pokhara, Nepal: Erythema MultiformeDocument56 pagesManipal College of Medical Sciences Pokhara, Nepal: Erythema MultiformeVaibhav KrishnaNo ratings yet
- VITILIGODocument21 pagesVITILIGOVaibhav KrishnaNo ratings yet
- Specific Types of DysnpeaDocument14 pagesSpecific Types of DysnpeaPiyush Agarwal100% (1)
- Acute Leukaemia Presentation 1Document20 pagesAcute Leukaemia Presentation 1Vaibhav KrishnaNo ratings yet
- Chest PainDocument23 pagesChest PainVaibhav KrishnaNo ratings yet
- UTI Tubulointerstitial DrugsDocument43 pagesUTI Tubulointerstitial DrugsVaibhav KrishnaNo ratings yet
- HIV in ChildrenDocument11 pagesHIV in ChildrenVaibhav KrishnaNo ratings yet
- LEUKEMIAsDocument56 pagesLEUKEMIAsVaibhav KrishnaNo ratings yet
- Kernicterus: Sahisnuta BasnetDocument10 pagesKernicterus: Sahisnuta BasnetVaibhav KrishnaNo ratings yet
- Approach To AnemiaDocument33 pagesApproach To AnemiaVaibhav KrishnaNo ratings yet
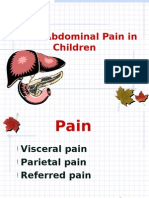
- Abdominal Pain in ChildrenDocument15 pagesAbdominal Pain in ChildrenVaibhav KrishnaNo ratings yet
- VSDDocument29 pagesVSDVaibhav Krishna100% (2)
- Anxiety DisorderDocument26 pagesAnxiety DisorderVaibhav KrishnaNo ratings yet
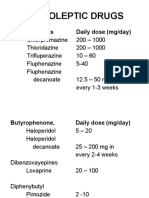
- Neuroleptic Drugs: Phenothiazines Daily Dose (Mg/day)Document11 pagesNeuroleptic Drugs: Phenothiazines Daily Dose (Mg/day)Vaibhav KrishnaNo ratings yet
- Schizophrenia: Disturbances Thinking in Feeling BehaviorDocument26 pagesSchizophrenia: Disturbances Thinking in Feeling BehaviorVaibhav KrishnaNo ratings yet
- Dissociation DisorderDocument33 pagesDissociation DisorderVaibhav KrishnaNo ratings yet
- 3rd Stage of LabourDocument16 pages3rd Stage of LabourVaibhav KrishnaNo ratings yet
- Antidepressants: I. Cyclic AntidepressantDocument17 pagesAntidepressants: I. Cyclic AntidepressantVaibhav KrishnaNo ratings yet
- Thyroid StormDocument33 pagesThyroid StormVaibhav Krishna50% (2)
- Shoulder DystociaDocument38 pagesShoulder DystociaVaibhav Krishna100% (1)
- Assessment of Loan Repayment Performance: in Case of Awash Bank in Sikela BranchDocument9 pagesAssessment of Loan Repayment Performance: in Case of Awash Bank in Sikela Branchbundesa buzo100% (1)
- Lembar Soal I. Read The Text Carefully and Choose The Best Answer Between A, B, C, D or E!Document5 pagesLembar Soal I. Read The Text Carefully and Choose The Best Answer Between A, B, C, D or E!nyunyunNo ratings yet
- V and D ReportDocument3 pagesV and D ReportkeekumaranNo ratings yet
- CFJ Seminars TrainingGuide L1EnglishDocument136 pagesCFJ Seminars TrainingGuide L1EnglishAttila AygininNo ratings yet
- 1001 Books I Must Read Before I DieDocument44 pages1001 Books I Must Read Before I DiemamaljNo ratings yet
- Katyusha Rocket LauncherDocument7 pagesKatyusha Rocket LauncherTepeRudeboyNo ratings yet
- Veer Singh RaghuvanshiDocument725 pagesVeer Singh RaghuvanshiDesi RocksNo ratings yet
- PhonemeDocument4 pagesPhonemealialim83No ratings yet
- Corporation True or FalseDocument2 pagesCorporation True or FalseAllyza Magtibay50% (2)
- How To Get Into Top IIMs - Ahmedabad, Bangalore, Calcutta and Lucknow - CareerAnnaDocument97 pagesHow To Get Into Top IIMs - Ahmedabad, Bangalore, Calcutta and Lucknow - CareerAnnaMoinak94No ratings yet
- Condo Contract of SaleDocument7 pagesCondo Contract of SaleAngelo MadridNo ratings yet
- Feminist Standpoint As Postmodern StrategyDocument21 pagesFeminist Standpoint As Postmodern StrategySumit AcharyaNo ratings yet
- The Constitution Con by Michael TsarionDocument32 pagesThe Constitution Con by Michael Tsarionsilent_weeper100% (1)
- Kangar 1 31/12/21Document4 pagesKangar 1 31/12/21TENGKU IRSALINA SYAHIRAH BINTI TENGKU MUHAIRI KTNNo ratings yet
- Gucci MurderDocument13 pagesGucci MurderPatsy StoneNo ratings yet
- Coursebook Answers Chapter 28 Asal ChemistryDocument3 pagesCoursebook Answers Chapter 28 Asal ChemistryAditiNo ratings yet
- Dairy IndustryDocument11 pagesDairy IndustryAbhishek SharmaNo ratings yet
- MAraguinot V Viva Films DigestDocument2 pagesMAraguinot V Viva Films DigestcattaczNo ratings yet
- Gravity & MagneticDocument13 pagesGravity & MagneticBunny Leal100% (1)
- Unity School of ChristianityDocument3 pagesUnity School of ChristianityServant Of TruthNo ratings yet
- B Blunt Hair Color Shine With Blunt: Sunny Sanjeev Masih PGDM 1 Roll No.50 Final PresentationDocument12 pagesB Blunt Hair Color Shine With Blunt: Sunny Sanjeev Masih PGDM 1 Roll No.50 Final PresentationAnkit Kumar SinghNo ratings yet
- Two Dimensional Flow of Water Through SoilDocument28 pagesTwo Dimensional Flow of Water Through SoilMinilik Tikur SewNo ratings yet
- Project Presentation (142311004) FinalDocument60 pagesProject Presentation (142311004) FinalSaad AhammadNo ratings yet
- Short StoriesDocument20 pagesShort StoriesPatrick Paul AlvaradoNo ratings yet
- Do 18-A and 18 SGV V de RaedtDocument15 pagesDo 18-A and 18 SGV V de RaedtThomas EdisonNo ratings yet
- 22 Habits of Unhappy PeopleDocument2 pages22 Habits of Unhappy PeopleKlEər OblimarNo ratings yet
- 34 The Aby Standard - CoatDocument5 pages34 The Aby Standard - CoatMustolih MusNo ratings yet
- Presentation2 Norman FosterDocument10 pagesPresentation2 Norman FosterAl JhanNo ratings yet
- Becg Unit-1Document8 pagesBecg Unit-1Bhaskaran Balamurali0% (1)