You might also like
- Testicular TorsionDocument20 pagesTesticular TorsionGAURAV100% (3)
- Lord Siva and His Worship by Swami SivanandaDocument236 pagesLord Siva and His Worship by Swami Sivanandakartikscribd100% (12)
- A System of Operative Surgery, Volume IV (of 4)From EverandA System of Operative Surgery, Volume IV (of 4)Rating: 4 out of 5 stars4/5 (1)
- Pancreatic Pseudocyst 2Document37 pagesPancreatic Pseudocyst 2AzharUlHassanQureshi100% (1)
- Enterocutaneous FistulaDocument34 pagesEnterocutaneous FistulaAkram ChalidNo ratings yet
- Small - Intestinal Neoplasms and Carcinoid TumorsDocument51 pagesSmall - Intestinal Neoplasms and Carcinoid TumorsOlga GoryachevaNo ratings yet
- 22.suture MaterialsDocument2 pages22.suture MaterialsShrestha AnjivNo ratings yet
- Acute Limb IschemiaDocument16 pagesAcute Limb IschemiaMohammad Husni BanisalmanNo ratings yet
- Testicular TorsionDocument24 pagesTesticular Torsionamal.fathullah100% (1)
- DVT Blok 4.1Document67 pagesDVT Blok 4.1Dz Putra100% (1)
- Fournier GangreneDocument16 pagesFournier GangreneAmirah Dahalan100% (1)
- Rule 21 SubpoenaDocument8 pagesRule 21 Subpoenacmv mendoza100% (1)
- TURP SyndromeDocument53 pagesTURP SyndromeElsya Paramitasari67% (3)
- Stoma Examination OSCE GuideDocument5 pagesStoma Examination OSCE GuideEssa AfridiNo ratings yet
- Principles of Non Operative Fracture ManagementDocument29 pagesPrinciples of Non Operative Fracture Managementronny100% (3)
- Negative Pressure Wound TherapyDocument21 pagesNegative Pressure Wound TherapyKathy Real Vills100% (2)
- Acute Abdomen and PeritonitisDocument17 pagesAcute Abdomen and PeritonitisAsuri KrishnaNo ratings yet
- Thoracic TraumaDocument77 pagesThoracic Traumasrtmedic92% (13)
- Abdominal Trauma: Supervised By: Dr. Hussein Al-HeisDocument63 pagesAbdominal Trauma: Supervised By: Dr. Hussein Al-HeisRashed ShatnawiNo ratings yet
- 6.examination of Inguinal SwellingDocument4 pages6.examination of Inguinal SwellingMuvenn Kannan100% (1)
- Endocrine Surgery: Butterworths International Medical Reviews: SurgeryFrom EverandEndocrine Surgery: Butterworths International Medical Reviews: SurgeryI. D. A. JohnstonNo ratings yet
- Law On Corporations Test Bank With Revised Corporate Code References - CompressDocument62 pagesLaw On Corporations Test Bank With Revised Corporate Code References - CompressCharles MateoNo ratings yet
- Pancreatic Cancer: Aziz Ahmad, MD Surgical Oncology Mills-Peninsula Hospital April 23, 2011Document18 pagesPancreatic Cancer: Aziz Ahmad, MD Surgical Oncology Mills-Peninsula Hospital April 23, 2011mywifenoor1983No ratings yet
- Penetrating Abdominal Trauma Emergency ManagementDocument29 pagesPenetrating Abdominal Trauma Emergency Managementanjali singhNo ratings yet
- Wound DebridementDocument53 pagesWound DebridementRahmat Arif Ayieb100% (1)
- Surgical Site InfectionsDocument52 pagesSurgical Site Infectionssahabatsalam07100% (5)
- LaparotomyDocument36 pagesLaparotomydenekeNo ratings yet
- Fat EmbolismDocument12 pagesFat EmbolismHastina HadnanNo ratings yet
- Pancreatitis: Dr. Ahmad Aqel RN, PHD The University of Jordan 2015Document27 pagesPancreatitis: Dr. Ahmad Aqel RN, PHD The University of Jordan 2015Anonymous 5HzElnmNo ratings yet
- TracheostomyDocument56 pagesTracheostomyRoshana MallawaarachchiNo ratings yet
- Orchidectomy Orchidopexy - NifDocument22 pagesOrchidectomy Orchidopexy - NifHamdan Yuwafi NaimNo ratings yet
- Presentation-Perianal AbscessDocument80 pagesPresentation-Perianal AbscessRommel Irabagon50% (2)
- Colon, Rectum and AnusDocument30 pagesColon, Rectum and AnusKiara GovenderNo ratings yet
- Damage Control SurgeryDocument31 pagesDamage Control SurgeryRose MendozaNo ratings yet
- Aetiology, Pathology and Management of Enterocutaneous FistulaDocument34 pagesAetiology, Pathology and Management of Enterocutaneous Fistularoselinekhadija100% (1)
- Updates in Management of Enterocutaneous FistulaDocument35 pagesUpdates in Management of Enterocutaneous FistulabashiruNo ratings yet
- Anal ProblemsDocument35 pagesAnal ProblemsSandip VaghelaNo ratings yet
- Central Venous LineDocument34 pagesCentral Venous Lineاسيرالاحزان100% (2)
- 6 Imaging of Acute AbdomenDocument73 pages6 Imaging of Acute AbdomenAliyah Tofani PawelloiNo ratings yet
- 7 Liver - Spleen TraumaDocument34 pages7 Liver - Spleen Traumabagus75% (4)
- TracheostomyDocument29 pagesTracheostomyFemi AustinNo ratings yet
- Dr. E. J. Arteen F.R.C.S General & Colorectal Consultant Surgeon European-Gaza HospitalDocument83 pagesDr. E. J. Arteen F.R.C.S General & Colorectal Consultant Surgeon European-Gaza Hospitalpt.mahmoudNo ratings yet
- Principles of OncologyDocument26 pagesPrinciples of OncologyDr Shahzad Alam ShahNo ratings yet
- Hydrocele, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHydrocele, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Gastrectomy 1Document86 pagesGastrectomy 1Mysnow OpalNo ratings yet
- Surgery - Pediatric GIT, Abdominal Wall, Neoplasms - 2014ADocument14 pagesSurgery - Pediatric GIT, Abdominal Wall, Neoplasms - 2014ATwinkle SalongaNo ratings yet
- Percutaneous Surgery of the Upper Urinary Tract: Handbook of EndourologyFrom EverandPercutaneous Surgery of the Upper Urinary Tract: Handbook of EndourologyPetrisor Aurelian GeavleteRating: 5 out of 5 stars5/5 (1)
- B43 Bristol Myers Company v. Director of Patents, GR L-21587, 19 May 1966, en Banc, Bengzon JP (J)Document1 pageB43 Bristol Myers Company v. Director of Patents, GR L-21587, 19 May 1966, en Banc, Bengzon JP (J)loschudentNo ratings yet
- Inguinal Hernia: Shohreh Toutounchi Reference: Schwartz Principles of Surgery 2010 Internship: 1391Document29 pagesInguinal Hernia: Shohreh Toutounchi Reference: Schwartz Principles of Surgery 2010 Internship: 1391Ritz CelsoNo ratings yet
- Anal Fissure: BY Alisha SaleemDocument7 pagesAnal Fissure: BY Alisha Saleemashar khanNo ratings yet
- In The Clinic - Acute PancreatitisDocument16 pagesIn The Clinic - Acute PancreatitisSurapon Nochaiwong100% (1)
- Intestinal Atresia and StenosisDocument7 pagesIntestinal Atresia and StenosisMichael NafarinNo ratings yet
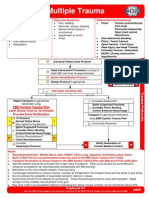
- Multiple Trauma ManagementDocument1 pageMultiple Trauma ManagementSetiawan Arif WibowoNo ratings yet
- Abdominal Compartment Syndrome: By: Adel Ghuloom, MD Lubna Kamaldien, MDDocument42 pagesAbdominal Compartment Syndrome: By: Adel Ghuloom, MD Lubna Kamaldien, MDnanang anacardia Subagyo100% (1)
- Surgical JaundiceDocument19 pagesSurgical JaundiceNur InsyirahNo ratings yet
- Acute AbdomenDocument24 pagesAcute AbdomenGrace SimmonsNo ratings yet
- Fat Embolism SyndromeDocument26 pagesFat Embolism SyndromeAzni MokhtarNo ratings yet
- Blunt Trauma AbdomenDocument41 pagesBlunt Trauma AbdomenSanthanu SukumaranNo ratings yet
- Wound de His Cence FinalDocument26 pagesWound de His Cence Finaldanil armandNo ratings yet
- Benign Tumors of The StomachDocument55 pagesBenign Tumors of The Stomachapi-19641337No ratings yet
- Preoperative Preparation of The Surgical PatientDocument33 pagesPreoperative Preparation of The Surgical PatientPrincewill SeiyefaNo ratings yet
- Fistula in AnoDocument3 pagesFistula in Anokhadzx80% (5)
- San Diego v. Hernandez DigestDocument1 pageSan Diego v. Hernandez DigestHanna QuiambaoNo ratings yet
- David OgilvyDocument5 pagesDavid OgilvyNiranjana ChandranNo ratings yet
- Computer Crimes (CCA CMA)Document81 pagesComputer Crimes (CCA CMA)Jerushah Jeet KaurNo ratings yet
- Imagery & Allusions in MacbethDocument9 pagesImagery & Allusions in MacbethGutsyNo ratings yet
- Unit 2: 1. Riser System 2. Sprinkler System 3. Spray SystemDocument11 pagesUnit 2: 1. Riser System 2. Sprinkler System 3. Spray Systemnimish ugemugeNo ratings yet
- San Mateo Daily Journal 03-16-19 EditionDocument32 pagesSan Mateo Daily Journal 03-16-19 EditionSan Mateo Daily JournalNo ratings yet
- Patagonia Finished Goods Supplier ListDocument6 pagesPatagonia Finished Goods Supplier ListHunter GeiselNo ratings yet
- Credit Memo - MH3M300182Document1 pageCredit Memo - MH3M300182AltafNo ratings yet
- Volume 47, Issue 48, November 25, 2016Document44 pagesVolume 47, Issue 48, November 25, 2016BladeNo ratings yet
- Sole Distribution AgreementDocument3 pagesSole Distribution AgreementNeal NilamNo ratings yet
- 5 - Agreement To Forfeit Real PropertyDocument8 pages5 - Agreement To Forfeit Real PropertyC BealeNo ratings yet
- Legal Pluralism: TH TH THDocument4 pagesLegal Pluralism: TH TH THNajwa HamdanNo ratings yet
- N-600, Application For Certificate of CitizenshipDocument0 pagesN-600, Application For Certificate of CitizenshipTaleen SakayanNo ratings yet
- Civil OrderDocument3 pagesCivil OrderAnne SchindlerNo ratings yet
- He 9780198767237 Chapter 20Document21 pagesHe 9780198767237 Chapter 20jaiahuja381No ratings yet
- Formi - How To Deal With Drunk FriendDocument2 pagesFormi - How To Deal With Drunk FriendHarshavardhan KRNo ratings yet
- International Human Rights Law Moot Court Respondent Argument by Amira Arkadia SetyaDocument3 pagesInternational Human Rights Law Moot Court Respondent Argument by Amira Arkadia SetyaAmiraNo ratings yet
- Gregorio, Forgive Us AllDocument3 pagesGregorio, Forgive Us AllNicole DilloNo ratings yet
- Capf 2014 FNRSLT EnglDocument5 pagesCapf 2014 FNRSLT EnglsagaravidayaNo ratings yet
- Final Leaflet BecDocument2 pagesFinal Leaflet Becthomas HambreNo ratings yet
- Legal Opinion Provincial Appraisal Committee CertificationDocument3 pagesLegal Opinion Provincial Appraisal Committee CertificationJohn Ludwig Bardoquillo PormentoNo ratings yet
- NankingDocument4 pagesNankingAlma ShamsNo ratings yet
- Case DigestDocument12 pagesCase DigestMARK TIMUGEN BELLANo ratings yet
- James Baldwin - Intro LessonDocument1 pageJames Baldwin - Intro LessonErwan KergallNo ratings yet
- B.A. (History) 2019-20Document20 pagesB.A. (History) 2019-20kunta kunta693No ratings yet
- Explosion of Light The White Horse and The Chariots IPH02Document6 pagesExplosion of Light The White Horse and The Chariots IPH02Tanya RonneNo ratings yet