You might also like
- Management of COPD in Primary and Secondary Care, TheFrom EverandManagement of COPD in Primary and Secondary Care, TheRating: 5 out of 5 stars5/5 (1)
- GOLD PocketGuide 2011 Jan18Document32 pagesGOLD PocketGuide 2011 Jan18Teresa ChangNo ratings yet
- AECOPD GuidelineDocument8 pagesAECOPD GuidelineRonlie RonneyNo ratings yet
- GOLD Pocket 2010mar31Document30 pagesGOLD Pocket 2010mar31Fatimah Az-zahraNo ratings yet
- Cmag CopdDocument83 pagesCmag CopdSofia MagalhaesNo ratings yet
- COPD2019Document9 pagesCOPD2019ClintonNo ratings yet
- Dpoc - Resumo Gold 2010Document30 pagesDpoc - Resumo Gold 2010Ana Luisa Souza PedreiraNo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD)Document7 pagesChronic Obstructive Pulmonary Disease (COPD)Dwight Lhenard TuazonNo ratings yet
- Jover Reflection PaperDocument2 pagesJover Reflection PaperGwen Myles JoverNo ratings yet
- Copd - 2 Penting 13Document14 pagesCopd - 2 Penting 13Rahmat MuliaNo ratings yet
- Gold Guidelines 2014 PDFDocument3 pagesGold Guidelines 2014 PDFKhalidNo ratings yet
- Annals EpocDocument16 pagesAnnals EpocewbNo ratings yet
- Copd Exacerbations in EdDocument23 pagesCopd Exacerbations in EdEzequiel MenesesNo ratings yet
- Gold Copd 2017Document4 pagesGold Copd 2017ChrisNo ratings yet
- COPD Guide: Diagnosis, Assessment, TreatmentDocument34 pagesCOPD Guide: Diagnosis, Assessment, TreatmentFa9v 1No ratings yet
- COPD Case Pres2Document29 pagesCOPD Case Pres2Kelly Queenie Andres100% (1)
- 2020 REPORT: Global Strategy For The Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary DiseaseDocument53 pages2020 REPORT: Global Strategy For The Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary DiseaseManoj GhimireNo ratings yet
- Artikel Ibnu Fiksani Riski - Bismillah FinishDocument5 pagesArtikel Ibnu Fiksani Riski - Bismillah FinishDidik PujiyantoNo ratings yet
- COPD Updated Guidelines and Newer TherapiesDocument90 pagesCOPD Updated Guidelines and Newer TherapiesVlad Constantin100% (1)
- COPD Clinical Management Review Provides GuidanceDocument11 pagesCOPD Clinical Management Review Provides GuidanceAlejandro Kanito Alvarez SNo ratings yet
- Key Points on Diagnosing and Assessing Severity of COPDDocument12 pagesKey Points on Diagnosing and Assessing Severity of COPDfallenczarNo ratings yet
- National Health Programs for Cardiovascular and Respiratory ConditionsDocument7 pagesNational Health Programs for Cardiovascular and Respiratory ConditionsJyoti singhNo ratings yet
- Spirometry in PracticeDocument24 pagesSpirometry in Practiceuser_at_scribd100% (1)
- Physiological Effects On SmokingDocument6 pagesPhysiological Effects On SmokingReyki Yudho HNo ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument28 pagesChronic Obstructive Pulmonary DiseaseZhe Kang LimNo ratings yet
- ??????? ??????????? ????????? ???????Document3 pages??????? ??????????? ????????? ???????Hạnh VũNo ratings yet
- 006 COPD - Lecture StudentsDocument52 pages006 COPD - Lecture Studentszyz6639No ratings yet
- BPOC in Medicina PrimaraDocument3 pagesBPOC in Medicina PrimaraAlina GheNo ratings yet
- Management of COPDDocument21 pagesManagement of COPDikrimahsbNo ratings yet
- GINA Pocket2013 May15Document0 pagesGINA Pocket2013 May15David BarzalloNo ratings yet
- PT Case: Copd Exacerbation: DedicationDocument10 pagesPT Case: Copd Exacerbation: DedicationDianaLopezBorjaNo ratings yet
- Review of Related LiteratureDocument4 pagesReview of Related LiteratureIvy Yvonne Quinico MalubagNo ratings yet
- Fumo 1Document10 pagesFumo 1Ailton Soares da Silva100% (1)
- Our Lady of Fatima University - ValenzuelaDocument3 pagesOur Lady of Fatima University - ValenzuelaMeriam Estepa MartinezNo ratings yet
- COPD CasepresentationDocument10 pagesCOPD CasepresentationSandra KartikaNo ratings yet
- Smoking and Respiratory DiseaseDocument5 pagesSmoking and Respiratory DiseaseIrfan FauziNo ratings yet
- Chronic Illness Module OutcomesDocument12 pagesChronic Illness Module OutcomesOmar IzzoNo ratings yet
- Copd Case StudyDocument6 pagesCopd Case StudyChrischia Yvonne GualbertoNo ratings yet
- Seminar (A5) - 1Document35 pagesSeminar (A5) - 1mohamed6j19No ratings yet
- Description: Back To TopDocument21 pagesDescription: Back To Toprovergzz88No ratings yet
- دکتر حسینی نیاDocument109 pagesدکتر حسینی نیاMasoud DoroodgarNo ratings yet
- Accepted Manuscript: SmokehazDocument40 pagesAccepted Manuscript: SmokehazyovanNo ratings yet
- Hemoptysis - CA Bronchus PDFDocument49 pagesHemoptysis - CA Bronchus PDFDarawan MirzaNo ratings yet
- Print 1Document8 pagesPrint 1Zaura Meliana MulyadiNo ratings yet
- COPD Management and PrognosisDocument21 pagesCOPD Management and PrognosisMudrekaNo ratings yet
- Acute Exacerbation of COPD Nursing Application of Evidence-Based GuidelinesDocument17 pagesAcute Exacerbation of COPD Nursing Application of Evidence-Based GuidelinesCandice ChengNo ratings yet
- Jurnal Respirasi PDFDocument14 pagesJurnal Respirasi PDFakhirul_733759154No ratings yet
- Copd PDFDocument28 pagesCopd PDFDarawan MirzaNo ratings yet
- D5W Uses and Side EffectsDocument4 pagesD5W Uses and Side EffectsHanilyn ArdinaNo ratings yet
- The Human Gut-Liver-Axis in Health and DiseaseFrom EverandThe Human Gut-Liver-Axis in Health and DiseaseAleksander KragNo ratings yet
- Topic 2 COPD and AsthmaDocument18 pagesTopic 2 COPD and AsthmaCaitlynNo ratings yet
- A Case Presentation On Chronic Obstructive Disease (COPD)Document18 pagesA Case Presentation On Chronic Obstructive Disease (COPD)Harvey T. Dato-onNo ratings yet
- Case Presentation On Copd - Shaik NazmaDocument29 pagesCase Presentation On Copd - Shaik NazmaDeepikaNo ratings yet
- Cigarette Smoking and Asthma: Clinical Management ReviewDocument15 pagesCigarette Smoking and Asthma: Clinical Management ReviewMuhammad FikriNo ratings yet
- Guideline On Management of Asthma in Adult and ChildrenDocument24 pagesGuideline On Management of Asthma in Adult and ChildrenJerry TanNo ratings yet
- PpokDocument6 pagesPpokSatria UtomoNo ratings yet
- The Management of Dental Patients with COPDDocument3 pagesThe Management of Dental Patients with COPDShirmayne TangNo ratings yet
- Bio-Ethical Issue and 3 ArticlesDocument7 pagesBio-Ethical Issue and 3 ArticlesSittie Nashieva A. UsmanNo ratings yet
- Managing Breathlessness in the CommunityFrom EverandManaging Breathlessness in the CommunityRating: 3.5 out of 5 stars3.5/5 (2)
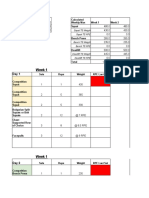
- Training Maxes and Weekly Workout LogsDocument45 pagesTraining Maxes and Weekly Workout LogsKönczölDávidNo ratings yet
- Nutrient-rich fish lumpia promotes children's developmentDocument3 pagesNutrient-rich fish lumpia promotes children's developmentBevelyn NaulNo ratings yet
- RRL and RrsDocument5 pagesRRL and RrsDwyane DelacernaNo ratings yet
- Penerapan NCP pada Pasien Hiperkolesterolemia Komplikasi HipertensiDocument9 pagesPenerapan NCP pada Pasien Hiperkolesterolemia Komplikasi HipertensiWidya SafitriNo ratings yet
- Ma de 101Document4 pagesMa de 101Quynh NguyenNo ratings yet
- Bucknell Strength Program for Intermediate LiftersDocument2 pagesBucknell Strength Program for Intermediate LiftersRyan PanNo ratings yet
- 20 Simple Ways To Fall Asleep Fast - Semeco, ADocument19 pages20 Simple Ways To Fall Asleep Fast - Semeco, ARoxan PacsayNo ratings yet
- Swift 2018Document33 pagesSwift 2018Sam Steven Hernandez JañaNo ratings yet
- Argumentative EssayDocument5 pagesArgumentative Essayapi-33103223333% (3)
- PE1 Lecture1Document26 pagesPE1 Lecture1Raphael Morante0% (1)
- Body Recomposition Training Program PDFDocument13 pagesBody Recomposition Training Program PDFvain glory100% (8)
- Nutrition in Adolescence Adulthood and ElderlyDocument62 pagesNutrition in Adolescence Adulthood and ElderlyZeheriahNo ratings yet
- TWO-Working Sheet Listening Activity Note TakingDocument6 pagesTWO-Working Sheet Listening Activity Note TakingFallih AllamNo ratings yet
- Calisthenics Program Basic AdvancedDocument30 pagesCalisthenics Program Basic Advancedjozsef10No ratings yet
- Cleveland City Council Ordinance For Flavored Tobacco BanDocument15 pagesCleveland City Council Ordinance For Flavored Tobacco BanWKYC.comNo ratings yet
- Benefits of BreastfeedingDocument2 pagesBenefits of BreastfeedingESPINOSA JHANNANo ratings yet
- Mrs Sill - Personalized Fitness PlanDocument26 pagesMrs Sill - Personalized Fitness PlanElisa Medina AlbinoNo ratings yet
- Get FREE meal plan, workout and FF30X guideDocument4 pagesGet FREE meal plan, workout and FF30X guidePaula Francisca FaríasNo ratings yet
- Ob PamphletDocument2 pagesOb Pamphletapi-305460281100% (3)
- Sleep Cycles - Stages - PsychologyDocument8 pagesSleep Cycles - Stages - PsychologyAshu BeniwalNo ratings yet
- Beginner's Health and Fitness GuideDocument19 pagesBeginner's Health and Fitness GuideDiana IonescuNo ratings yet
- Mood ChartDocument2 pagesMood ChartDanielle DonahueNo ratings yet
- C.H.A. Diet - Vol.2Document62 pagesC.H.A. Diet - Vol.2Sixp8ck100% (3)
- Nutritional Status of Filipino ChildrenDocument20 pagesNutritional Status of Filipino ChildrenCar OrdzNo ratings yet
- Research Proposal ExampleDocument3 pagesResearch Proposal Exampleapi-339321505100% (1)
- The 70s Bulk, Tall Man Edition 2020 v2Document30 pagesThe 70s Bulk, Tall Man Edition 2020 v2lorenzoNo ratings yet
- Q4 PE 9 Week8Document4 pagesQ4 PE 9 Week8Kim Carlo Tunay IsletaNo ratings yet
- Nutrition PowerpointDocument22 pagesNutrition Powerpointasdkl1234No ratings yet
- Effect of Nutrition Education On Knowledge, Complementary Feeding, and Hygiene Practices of Mothers With Moderate Acutely Malnourished Children in UgandaDocument10 pagesEffect of Nutrition Education On Knowledge, Complementary Feeding, and Hygiene Practices of Mothers With Moderate Acutely Malnourished Children in Ugandalinlin lindayaniNo ratings yet
- Product Training Guide PDFDocument3 pagesProduct Training Guide PDFNicol Iulia GurăuNo ratings yet