You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Physical Assessment Guide of Head-To-ToeDocument9 pagesPhysical Assessment Guide of Head-To-Toeneleh gray100% (2)
- Art of Public Speaking 12th Edition Stephen Lucas Test Bank DownloadDocument34 pagesArt of Public Speaking 12th Edition Stephen Lucas Test Bank DownloadCheryl Crigger100% (24)
- The Importance of Sound Design on PerceptionDocument48 pagesThe Importance of Sound Design on PerceptiondoeditNo ratings yet
- Nursing Interventions for Anxiety and Psychiatric DisordersDocument32 pagesNursing Interventions for Anxiety and Psychiatric DisordersJohn Lyndon Sayong100% (3)
- Flunarizine Effective Migrainous Vertigo PreventionDocument6 pagesFlunarizine Effective Migrainous Vertigo PreventionNanda WtNo ratings yet
- A Comparative Effectiveness Meta-Analysis of Drugs For The Prophylaxis of Migraine HeadacheDocument60 pagesA Comparative Effectiveness Meta-Analysis of Drugs For The Prophylaxis of Migraine HeadachetriaclaresiaNo ratings yet
- Tugas Ekspertise AbdomenDocument42 pagesTugas Ekspertise AbdomentriaclaresiaNo ratings yet
- Oxygen For Cluster Headaches: A GuideDocument25 pagesOxygen For Cluster Headaches: A GuidetriaclaresiaNo ratings yet
- De-Regil Et Al-2016-The Cochrane LibraryDocument124 pagesDe-Regil Et Al-2016-The Cochrane LibrarytriaclaresiaNo ratings yet
- Creamer Et Al-2016-British Journal of DermatologyDocument34 pagesCreamer Et Al-2016-British Journal of DermatologyAtika Indah SariNo ratings yet
- Initial Severity of Schizophrenia and EfficacyDocument20 pagesInitial Severity of Schizophrenia and EfficacytriaclaresiaNo ratings yet
- E. HystoliticaDocument7 pagesE. HystoliticatriaclaresiaNo ratings yet
- Supplementation of Vitamin D in Pregnancy and Its Correlation With Feto-Maternal OutcomeDocument20 pagesSupplementation of Vitamin D in Pregnancy and Its Correlation With Feto-Maternal OutcometriaclaresiaNo ratings yet
- Benign Paroxysmal Positional VertigoDocument65 pagesBenign Paroxysmal Positional VertigoReni SusantiNo ratings yet
- Yoi 140088Document779 pagesYoi 140088triaclaresiaNo ratings yet
- Perioperative Dextromethorphan As An Adjunct For Postoperative PainDocument10 pagesPerioperative Dextromethorphan As An Adjunct For Postoperative PaintriaclaresiaNo ratings yet
- Introduction To Serology - Immunology, HSV & H.pyloriDocument37 pagesIntroduction To Serology - Immunology, HSV & H.pyloritriaclaresiaNo ratings yet
- Guidelines For The Administration of Blood and Blood ComponentsDocument29 pagesGuidelines For The Administration of Blood and Blood ComponentsCindya PerthyNo ratings yet
- Clinical Use of BloodDocument221 pagesClinical Use of BloodRizma Adlia100% (1)
- BPPVDocument36 pagesBPPVRizka AmaliaNo ratings yet
- Panss ScoreDocument8 pagesPanss ScoretriaclaresiaNo ratings yet
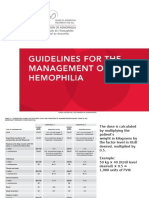
- Dosis HemofiliaDocument5 pagesDosis HemofiliatriaclaresiaNo ratings yet
- S1 Diet, Immune and InfectionDocument48 pagesS1 Diet, Immune and InfectiontriaclaresiaNo ratings yet
- Anasurgery MockboardDocument12 pagesAnasurgery MockboardVince CabahugNo ratings yet
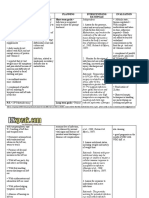
- Otitis Media Nurisng Care PlanDocument11 pagesOtitis Media Nurisng Care PlanRnspeakcom100% (1)
- NURS 336-Fall-2020-OutlineDocument5 pagesNURS 336-Fall-2020-OutlineyuddNo ratings yet
- (Inc. Barcharts) Senses Laminated Reference Guide (Z Lib - Org)Document2 pages(Inc. Barcharts) Senses Laminated Reference Guide (Z Lib - Org)Camilo Ignacio Arriagada Jara100% (1)
- Anatomy and PhysiologyDocument138 pagesAnatomy and PhysiologyMikee GatlabayanNo ratings yet
- Ear AssessmentDocument23 pagesEar AssessmentRotsen B. VelascoNo ratings yet
- Kel. 1Document29 pagesKel. 1Alisha Putri SetianiNo ratings yet
- History Pe EntDocument44 pagesHistory Pe EntFalling HateNo ratings yet
- Hydrops and Menieres DietDocument3 pagesHydrops and Menieres DietclaitonborgesNo ratings yet
- Multiple Choice Questions: A. B. C. DDocument37 pagesMultiple Choice Questions: A. B. C. DwanderagroNo ratings yet
- By MBBS Gang: ENT Examination ProcedureDocument23 pagesBy MBBS Gang: ENT Examination ProcedureYour DaddyNo ratings yet
- Photonicsspectra 201208Document84 pagesPhotonicsspectra 201208denghueiNo ratings yet
- Multiple Choice QuestionsDocument29 pagesMultiple Choice Questionsfatimaawan8989No ratings yet
- Mastoidectomy: Surgical Techniques: Key PointsDocument14 pagesMastoidectomy: Surgical Techniques: Key PointsMichel Dayanna Serrano TasconNo ratings yet
- Physiology of Hearing in 40 CharactersDocument12 pagesPhysiology of Hearing in 40 CharactersMusarrat NazeerNo ratings yet
- Meniere's DiseaseDocument50 pagesMeniere's DiseaseRaisa CleizeraNo ratings yet
- Literature Reading on Cochlear ImplantsDocument35 pagesLiterature Reading on Cochlear ImplantsOke KadarullahNo ratings yet
- Hearing Aid ManualDocument54 pagesHearing Aid Manualapi-529618960No ratings yet
- CBSE Class 9 Science Chapter 12 Sound Back QuestionsDocument7 pagesCBSE Class 9 Science Chapter 12 Sound Back QuestionsRavi Ranjan SinghNo ratings yet
- Sensory Receptors Sensory Receptors: ExteroreceptorsDocument10 pagesSensory Receptors Sensory Receptors: ExteroreceptorsMikhail CarvalhoNo ratings yet
- Medical Certificate For Service at Sea: ConfidentialDocument4 pagesMedical Certificate For Service at Sea: ConfidentialADMIN MCU RSU SAHID SAHIRMAN100% (1)
- Class 7Document5 pagesClass 7Wahid Bashir100% (4)
- Summative AssessmentDocument3 pagesSummative Assessmentapi-383086643No ratings yet
- Gregorian HealthDocument5 pagesGregorian HealthChristina MendozaNo ratings yet
- p1713 PDFDocument8 pagesp1713 PDFfunnie175No ratings yet
- Oleson2014-Auricle Accupuncture NomenclatureDocument15 pagesOleson2014-Auricle Accupuncture NomenclaturebillNo ratings yet