You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- TegarDOPS DR LusitoDocument3 pagesTegarDOPS DR LusitoImada KhoironiNo ratings yet
- Jurnal InternaDocument6 pagesJurnal InternaImada KhoironiNo ratings yet
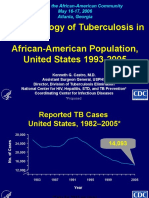
- Epidemiology of Tuberculosis in African-American Population, United States 1993-2005Document20 pagesEpidemiology of Tuberculosis in African-American Population, United States 1993-2005Imada KhoironiNo ratings yet
- Pemeriksaan Thorax: Coass Interna RSI Sultan Agung SemarangDocument59 pagesPemeriksaan Thorax: Coass Interna RSI Sultan Agung SemarangImada KhoironiNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- AVSD - Revised VersionDocument3 pagesAVSD - Revised Versiondr_IstiqlalMiftahulJannahNo ratings yet
- The Radiology Assistant - Coronary Anatomy and Anomalies PDFDocument7 pagesThe Radiology Assistant - Coronary Anatomy and Anomalies PDFUlilta MuktadiraNo ratings yet
- Congestive Cardiac Failure PDFDocument28 pagesCongestive Cardiac Failure PDFNANDHINI S100% (1)
- Label The Circulatory SystemDocument2 pagesLabel The Circulatory SystemIzzu PenielNo ratings yet
- Mitral Stenosis and Mitral RegurgitationDocument21 pagesMitral Stenosis and Mitral Regurgitationash_wan88No ratings yet
- Inspection and Palpation of The HeartDocument38 pagesInspection and Palpation of The Heartstudymedic100% (2)
- The Heart: Dr. Silvia BoyajianDocument44 pagesThe Heart: Dr. Silvia BoyajianAsem YousefNo ratings yet
- (Medicalstudyzone - Com) NBME 25 Answers VersionDocument200 pages(Medicalstudyzone - Com) NBME 25 Answers VersionMahnoor Tauqeer100% (1)
- Congenital Heart DiseaseDocument2 pagesCongenital Heart DiseaseFrancis GacheruNo ratings yet
- Neurogenic and Myogenic HeartsDocument14 pagesNeurogenic and Myogenic HeartsYCMOUNo ratings yet
- 5.pleural CavitiesDocument6 pages5.pleural CavitiesAmrith LordNo ratings yet
- Anatomy - Posterior Triangle of The Neck PDFDocument4 pagesAnatomy - Posterior Triangle of The Neck PDFAngel Kim100% (1)
- Unit 6 Part 2 Thoracic CavityDocument56 pagesUnit 6 Part 2 Thoracic CavitySiraj ShiferawNo ratings yet
- Transesophageal Echocardiography: M. Elizabeth Brickner, MDDocument9 pagesTransesophageal Echocardiography: M. Elizabeth Brickner, MDHilario. Hayascent.Reign.M.No ratings yet
- Intercostal SpaceDocument38 pagesIntercostal SpaceDrravikumar BhandariNo ratings yet
- The Final FRCR Complete Revision Notes-Pages-Deleted - PagenumberDocument364 pagesThe Final FRCR Complete Revision Notes-Pages-Deleted - PagenumberObaidy AlbushaherNo ratings yet
- BuaDocument3 pagesBuaAnonymous xyaZgBmRNo ratings yet
- 227 Full PDFDocument3 pages227 Full PDFanon_629352389No ratings yet
- Systemic and Pulmonary CirculationDocument13 pagesSystemic and Pulmonary CirculationLuis eduardo bolaño vilaNo ratings yet
- Echocardiography in Heart Failure: A Guide For General PracticeDocument6 pagesEchocardiography in Heart Failure: A Guide For General PracticesavitageraNo ratings yet
- Acute STEMI With Multiple Culprit Vessels in Young MaleDocument24 pagesAcute STEMI With Multiple Culprit Vessels in Young MaleVickry WahidjiNo ratings yet
- Defenisi: Terdapatnya Cairan DLM Rongga Pleura Terjadinya: GGN Absorbsi & Reabsorbsi Cairan Pleura PatogenesisDocument16 pagesDefenisi: Terdapatnya Cairan DLM Rongga Pleura Terjadinya: GGN Absorbsi & Reabsorbsi Cairan Pleura PatogenesisAlimMarsNo ratings yet
- Examinarea Clinică in Afecţiuni Ale Aparatului CardiovascularDocument49 pagesExaminarea Clinică in Afecţiuni Ale Aparatului CardiovascularFranceska LtkNo ratings yet
- Blood Supply of HeartDocument20 pagesBlood Supply of HeartPraneethaNo ratings yet
- Correlative Anatomy For The Electrophysiologist, Part I:: The Pericardial Space, Oblique Sinus, Transverse SinusDocument6 pagesCorrelative Anatomy For The Electrophysiologist, Part I:: The Pericardial Space, Oblique Sinus, Transverse Sinusaldi akbarNo ratings yet
- Parts of The HeartDocument18 pagesParts of The HeartCHRISTOPHER FAYLONNo ratings yet
- How To Interpret An Echocardiography Report (For The Non-Imager) ?Document12 pagesHow To Interpret An Echocardiography Report (For The Non-Imager) ?VandeosNo ratings yet
- Radcliffe EducationDocument4 pagesRadcliffe EducationSherwin Buenavente SulitNo ratings yet
- LDC by Transit RuleDocument49 pagesLDC by Transit RuleRenz Janfort Junsay Graganza100% (1)
- Thoraxic WallDocument13 pagesThoraxic WallandiedeeNo ratings yet