You might also like
- High Protein & Low Carb Diet Women - Lose Weight Quickly and Much - Men - Increase Muscle Mass and Become Very Strong -: COOKBOOK, #3From EverandHigh Protein & Low Carb Diet Women - Lose Weight Quickly and Much - Men - Increase Muscle Mass and Become Very Strong -: COOKBOOK, #3No ratings yet
- For The Surgical Patient: Kelly Sparks LDN, RDDocument47 pagesFor The Surgical Patient: Kelly Sparks LDN, RDManikandaprabhu sivaNo ratings yet
- Ketogenic Diet : No Sugar No Starch Diet To Turn Your Fat Into Energy In 7 Days (Bonus : 50 Easy Recipes To Jump Start Your Fat & Low Carb Weight Loss Today)From EverandKetogenic Diet : No Sugar No Starch Diet To Turn Your Fat Into Energy In 7 Days (Bonus : 50 Easy Recipes To Jump Start Your Fat & Low Carb Weight Loss Today)Rating: 3.5 out of 5 stars3.5/5 (4)
- Nutrition: - . - and The Surgical PatientDocument39 pagesNutrition: - . - and The Surgical PatientJan Cyrill YuNo ratings yet
- Impact of Surgical Nutrition on Patient OutcomesDocument54 pagesImpact of Surgical Nutrition on Patient OutcomesAmir SharifNo ratings yet
- Nutrition Support Surgical PatientsDocument35 pagesNutrition Support Surgical PatientsFuad Aman AbjNo ratings yet
- Nutrition in SurgeryDocument23 pagesNutrition in SurgeryJayaram PandeyNo ratings yet
- Nutrition PostoperativeDocument47 pagesNutrition PostoperativeAnonymous 86gki5No ratings yet
- Nutrition in SurgeryDocument49 pagesNutrition in SurgeryIswaran AmpalakanNo ratings yet
- Nutrition in CirrhosisDocument40 pagesNutrition in CirrhosisAuliangi TamayoNo ratings yet
- Nutrition in Surgical PatientDocument26 pagesNutrition in Surgical Patient180045No ratings yet
- 01 Enteral and Parenteral Nutrition Support PSIK UMMDocument68 pages01 Enteral and Parenteral Nutrition Support PSIK UMMSri YulianaNo ratings yet
- Essential Enteral and Parenteral Nutrition GuideDocument64 pagesEssential Enteral and Parenteral Nutrition GuideHeba IyadNo ratings yet
- Vitamin B12 Deficiency and A Patient Case StudyDocument36 pagesVitamin B12 Deficiency and A Patient Case Studynherm6425100% (1)
- Surgical Nutrition For MS Part 1 Peradeniya March 2007Document38 pagesSurgical Nutrition For MS Part 1 Peradeniya March 2007Chamika HuruggamuwaNo ratings yet
- Enteral Nutrition GI Disorders - Olivier GouletDocument60 pagesEnteral Nutrition GI Disorders - Olivier GouletBayu KurniawanNo ratings yet
- Surgical Nutritions: Prepared By: Lilibeth C.Tenorio, M.DDocument33 pagesSurgical Nutritions: Prepared By: Lilibeth C.Tenorio, M.DLilibeth Tenorio De Leon100% (1)
- Nutrition Support: Sean P Harbison MDDocument42 pagesNutrition Support: Sean P Harbison MDsgod34No ratings yet
- Enteral Nutrition: Agus PrastowoDocument49 pagesEnteral Nutrition: Agus Prastowokartika sariNo ratings yet
- Everything You Need to Know About Parenteral NutritionDocument31 pagesEverything You Need to Know About Parenteral NutritionNicholas PetrovskiNo ratings yet
- Lecture On en and PNDocument92 pagesLecture On en and PNJerrold CruzNo ratings yet
- Parenteral Nutrition: DR Mohd Nikman AhmadDocument35 pagesParenteral Nutrition: DR Mohd Nikman AhmadMaryGraceVelascoFuentesNo ratings yet
- They Help in CholesterolDocument82 pagesThey Help in CholesterolEileen del RosarioNo ratings yet
- TPNDocument57 pagesTPNPeace Andong PerochoNo ratings yet
- Shafer Oncology Case StudyDocument21 pagesShafer Oncology Case Studyapi-307506037No ratings yet
- ISC Workshop - Surgical Nutrition and Fluid and Electrolytes - 2010Document58 pagesISC Workshop - Surgical Nutrition and Fluid and Electrolytes - 2010fiansisNo ratings yet
- Transdermal Drug Delivery SystemDocument99 pagesTransdermal Drug Delivery SystemIshtiaq AhmedNo ratings yet
- Management Short Bowel - Duerksen RamanDocument67 pagesManagement Short Bowel - Duerksen RamandavidwheelerNo ratings yet
- Nutrition in Sick PatientsDocument50 pagesNutrition in Sick PatientsIbnu ZakiNo ratings yet
- 10 Diet and Nutrition For Liver Disease and HepatitisDocument71 pages10 Diet and Nutrition For Liver Disease and HepatitisMubark Al AwlaqyNo ratings yet
- Equilíbrio Veterinary Product KnowledgeDocument141 pagesEquilíbrio Veterinary Product KnowledgeDerlin NahariNo ratings yet
- Nutrition: - . - and The Surgical Patient (Pre and Post Operative Nutrition)Document58 pagesNutrition: - . - and The Surgical Patient (Pre and Post Operative Nutrition)SanaSofiyahNo ratings yet
- MEDICAL NUTRITION THERAPY FOR RENAL DISEASEDocument39 pagesMEDICAL NUTRITION THERAPY FOR RENAL DISEASESteven FongNo ratings yet
- FALL 2021 N41A Basic Nutrition TherapyDocument44 pagesFALL 2021 N41A Basic Nutrition TherapyheliNo ratings yet
- I GD Tuban Eling Tulus WDocument24 pagesI GD Tuban Eling Tulus WputriNo ratings yet
- Perforated Duodenal Ulcer Case StudyDocument45 pagesPerforated Duodenal Ulcer Case StudyJijie AzeeraNo ratings yet
- Metabolism in SurgeryDocument5 pagesMetabolism in Surgeryjc_sibal13No ratings yet
- Nutrition in BurnsDocument27 pagesNutrition in BurnsRaghuram PrasadNo ratings yet
- Nutritional Interventions in Critical IllnessDocument10 pagesNutritional Interventions in Critical IllnessGigo4infinityNo ratings yet
- TPNDocument69 pagesTPNMylz MendozaNo ratings yet
- Enteral & Parenteral FeedingDocument36 pagesEnteral & Parenteral FeedingWahono Ahon Wahyu Al-FatihNo ratings yet
- Clinical Case Report Powerpoint PresentationDocument24 pagesClinical Case Report Powerpoint Presentationapi-354139540100% (1)
- 502 A 71 D 0 Ec 4 B 7 C 7 BCB 12Document7 pages502 A 71 D 0 Ec 4 B 7 C 7 BCB 12api-464193636No ratings yet
- SURGICAL NUTRITION GUIDEDocument59 pagesSURGICAL NUTRITION GUIDEPrincewill SeiyefaNo ratings yet
- Nutritional Managements of Gastrointestinal Diseases/DisordersDocument54 pagesNutritional Managements of Gastrointestinal Diseases/Disordersendang sry09No ratings yet
- Nutritional Management for Patients with Chronic Kidney DiseaseDocument41 pagesNutritional Management for Patients with Chronic Kidney DiseaseZaza ZunitaNo ratings yet
- Kuliah Blok Growth and DevelopmentDocument44 pagesKuliah Blok Growth and Developmentjaish8904No ratings yet
- Case StudyDocument5 pagesCase Studyapi-247850107No ratings yet
- Prescribing Regimens of Feeding JejunostomyDocument28 pagesPrescribing Regimens of Feeding JejunostomyRajarshi KumarNo ratings yet
- Meet B.G.: A Nutrition Care Plan by Michelle SartaDocument14 pagesMeet B.G.: A Nutrition Care Plan by Michelle Sartaapi-340851914No ratings yet
- Entral NutritionDocument73 pagesEntral NutritionAmr OthmanNo ratings yet
- Nutrition in Ped CCM (Picucourse)Document46 pagesNutrition in Ped CCM (Picucourse)surasuarezlopezNo ratings yet
- Nutritional Support in ICU Patient TMKDocument61 pagesNutritional Support in ICU Patient TMKhabtsh habshaNo ratings yet
- NZR TPN PrabuDocument56 pagesNZR TPN PrabuikesesariaNo ratings yet
- Cystic Fibrosis Case StudyDocument27 pagesCystic Fibrosis Case StudyMegan100% (5)
- Enteral Nutrition GuideDocument38 pagesEnteral Nutrition GuideWidi Alya ZhafiraNo ratings yet
- Lecture 8 Nutrition Enteral and ParenteralDocument42 pagesLecture 8 Nutrition Enteral and Parenteraljaish8904No ratings yet
- 3 1 14 Nutritional-SupportDocument2 pages3 1 14 Nutritional-SupportNi Wayan Ana PsNo ratings yet
- Short Bowel SyndromeDocument50 pagesShort Bowel SyndromeAbdul QadirNo ratings yet
- Article 154 - Allergic Gastroenteritis-Feline - 0Document2 pagesArticle 154 - Allergic Gastroenteritis-Feline - 0Steffany VanegasNo ratings yet
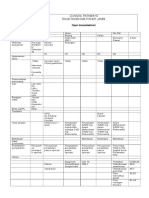
- Clinical Pathway Open CholecystektomiDocument2 pagesClinical Pathway Open CholecystektomiAnton TrihartantoNo ratings yet
- Rjpo - JF - Maret 2011Document62 pagesRjpo - JF - Maret 2011Mell-JasmineNo ratings yet
- Beauty V ShapeDocument22 pagesBeauty V ShapeMell-Jasmine50% (2)
- Beautiful Secrets After Birth: Dr. Melati - Esther House of BeautyDocument10 pagesBeautiful Secrets After Birth: Dr. Melati - Esther House of BeautyMell-JasmineNo ratings yet
- PRISMA 2009 Checklist: An AnalysisDocument2 pagesPRISMA 2009 Checklist: An AnalysisFiŗåš ÀßßâşNo ratings yet
- CaspDocument3 pagesCaspMell-JasmineNo ratings yet
- Mis Cursos: Área Personal E6D2NV Tema 1 Use of LanguageDocument8 pagesMis Cursos: Área Personal E6D2NV Tema 1 Use of LanguagePriscila ManjarreNo ratings yet
- Guess Papers For FmgeDocument34 pagesGuess Papers For FmgeSharat ChandraNo ratings yet
- Chettinad Hospital & Research Institue (A Unit of Care) : Clinical Laboratory - BiochemistryDocument2 pagesChettinad Hospital & Research Institue (A Unit of Care) : Clinical Laboratory - Biochemistryvaseem1981No ratings yet
- Nephrology MCQSDocument16 pagesNephrology MCQSThana AlAnsari100% (5)
- Nutritional status of type 2 diabetes patients based on anthropometryDocument7 pagesNutritional status of type 2 diabetes patients based on anthropometryIntan PratiwiNo ratings yet
- ESC Guidelines Heart Failure 2012Document61 pagesESC Guidelines Heart Failure 2012igohNo ratings yet
- Fitness Chart: Trek The HimalayasDocument1 pageFitness Chart: Trek The Himalayaspradnya7289No ratings yet
- Prevalence and Correlates of Adolescent Obesity Among Young Adults in South-Western NigeriaDocument12 pagesPrevalence and Correlates of Adolescent Obesity Among Young Adults in South-Western Nigeriaijmb333No ratings yet
- 15 CH110 Lipids TimberlakeDocument96 pages15 CH110 Lipids TimberlakeSumit TatedNo ratings yet
- Ruminant Physiology - Digestion, Metabolism, Growth and ReproductionDocument472 pagesRuminant Physiology - Digestion, Metabolism, Growth and ReproductionWendell Fellipe BaiaNo ratings yet
- Anti-Diet by Christy HarrisonDocument223 pagesAnti-Diet by Christy HarrisonTu Nutriguia90% (29)
- Hypokalaemia and Hypertension CausesDocument44 pagesHypokalaemia and Hypertension Causeslestrange1984100% (1)
- Classic Abs Training ReportDocument22 pagesClassic Abs Training ReportVikas Goyal100% (2)
- 10 Intriguing Facts About Ancient EgyptDocument5 pages10 Intriguing Facts About Ancient EgyptDiana LarisaNo ratings yet
- TYPES OF EATINGDocument2 pagesTYPES OF EATINGArdelia B. Vidal100% (1)
- A Proposal Sample TemplateDocument4 pagesA Proposal Sample Templateapi-356642645No ratings yet
- (Human Health Handbooks) Caroline Hollins-Martin, Olga Van Den Akker, Colin Martin, Victor R. Preedy-Handbook of Diet and Nutrition in The Menstrual Cycle, Periconception and Fertility-Wageningen PersDocument569 pages(Human Health Handbooks) Caroline Hollins-Martin, Olga Van Den Akker, Colin Martin, Victor R. Preedy-Handbook of Diet and Nutrition in The Menstrual Cycle, Periconception and Fertility-Wageningen PersSeeranga Chetty Raghunathan100% (2)
- NBME Practice Test 2 Pt. 2Document13 pagesNBME Practice Test 2 Pt. 2Zoë IndigoNo ratings yet
- Reviewer in Peh 1 1st QuarterDocument8 pagesReviewer in Peh 1 1st QuarterallyNo ratings yet
- PE12 Q2 Module5Document20 pagesPE12 Q2 Module5Kevin Bautista TamayoNo ratings yet
- Calisthenics Transformation - Body Weight TransformationDocument1 pageCalisthenics Transformation - Body Weight TransformationShahbaz SyedNo ratings yet
- ThePaleoApproach List of Autoimmune DiseasesDocument3 pagesThePaleoApproach List of Autoimmune DiseasesdevabakhtiNo ratings yet
- Assessment of Nutritional Status of People Living With HIV/AIDS (PLWHA) in The Age Group of 18-55 YearsDocument12 pagesAssessment of Nutritional Status of People Living With HIV/AIDS (PLWHA) in The Age Group of 18-55 YearsIOSRjournalNo ratings yet
- 3 Step NutritionDocument12 pages3 Step NutritionIonut Chicinas100% (1)
- Congestive Heart Failure (CHF) PDFDocument2 pagesCongestive Heart Failure (CHF) PDFZazulizer Are BackNo ratings yet
- Fmed 05 00160Document28 pagesFmed 05 00160Cristina Saldias PorrasNo ratings yet
- Vce Physical Education Unit OutlineDocument11 pagesVce Physical Education Unit Outlineapi-328688284No ratings yet
- Lunch Bunch - Kids Healthy Options ProgrammeDocument7 pagesLunch Bunch - Kids Healthy Options ProgrammeAlison Hourihan - Nutrition Division100% (2)
- Homework Lesson 2Document10 pagesHomework Lesson 2vanhung2809No ratings yet
- Functional Foods: Presented To: Ms Rabia Presented By: Amna AdilDocument10 pagesFunctional Foods: Presented To: Ms Rabia Presented By: Amna AdilAMNA ADILNo ratings yet