You might also like
- Pathology Mechanism: Jefferson Fracture Is The Eponymous Name Given To A Burst Fracture ofDocument25 pagesPathology Mechanism: Jefferson Fracture Is The Eponymous Name Given To A Burst Fracture ofAtikah FairuzNo ratings yet
- Cervical Spine FracturesDocument74 pagesCervical Spine FracturessrhubanbabuNo ratings yet
- Spinal Cord InjuryDocument13 pagesSpinal Cord Injurypaul_allan17No ratings yet
- Spinal Cord Injury (SCI)Document14 pagesSpinal Cord Injury (SCI)Joanna TaylanNo ratings yet
- Spinal Cord Injury: Presented By: Feliciano, Jenard R. Flores, Arliah Q. Gaspar, Danica VDocument79 pagesSpinal Cord Injury: Presented By: Feliciano, Jenard R. Flores, Arliah Q. Gaspar, Danica VPam RomeroNo ratings yet
- Spinal Cord Injury: C M, S - P J - LDocument99 pagesSpinal Cord Injury: C M, S - P J - Lsheel1No ratings yet
- Acute Spinal Cord CompressionDocument13 pagesAcute Spinal Cord CompressionWhoNo ratings yet
- Spinal Cord InjuryDocument16 pagesSpinal Cord Injuryjohnlester_jlf100% (2)
- Spinal Cord InjuryDocument17 pagesSpinal Cord InjurygireeshsachinNo ratings yet
- Spinal Cord InjuryDocument18 pagesSpinal Cord Injuryfaye kimNo ratings yet
- طب باطني (نظري) م8Document4 pagesطب باطني (نظري) م8asalla.fayyad.rdNo ratings yet
- Spinal Cord Injury NotesDocument13 pagesSpinal Cord Injury Notescorememories10No ratings yet
- Spinal Injuries: DR Abdelmoniem SaeedDocument44 pagesSpinal Injuries: DR Abdelmoniem SaeedYousef Al-AmeenNo ratings yet
- Spinal Cord Injuries-KyienDocument25 pagesSpinal Cord Injuries-KyienjohnnyienNo ratings yet
- Brachial Plexus InjuryDocument8 pagesBrachial Plexus InjurylewienNo ratings yet
- LWBK836 Ch123 p1332-1339Document8 pagesLWBK836 Ch123 p1332-1339metasoniko81No ratings yet
- Evaluation and Management of Acute Cervical Spine Trauma-RKY-finalDocument84 pagesEvaluation and Management of Acute Cervical Spine Trauma-RKY-finalRickky MDNo ratings yet
- C2 (Axis) FracturesDocument12 pagesC2 (Axis) FracturesSetyo Budi Premiaji WidodoNo ratings yet
- LP SpinalDocument11 pagesLP SpinalHimaniNo ratings yet
- Neck Trauma, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandNeck Trauma, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Lesion Del Tracto Cortico - Espinal InglesDocument14 pagesLesion Del Tracto Cortico - Espinal InglesCarolina Andrea Daza CharrisNo ratings yet
- Spinal Cord Injury NotesDocument13 pagesSpinal Cord Injury Notescorememories10No ratings yet
- Spinal Cord InjuryDocument24 pagesSpinal Cord InjurySteph VistalNo ratings yet
- Anatomy of Spinal CordDocument43 pagesAnatomy of Spinal CordGargi MPNo ratings yet
- Thoracolumbarfractures 150817055817 Lva1 App6891Document75 pagesThoracolumbarfractures 150817055817 Lva1 App6891Pap PipNo ratings yet
- Spinal Cord InjuryDocument12 pagesSpinal Cord InjuryAhmed Al-arapyNo ratings yet
- Clinical Neurology Prepared By: Utkarsha and Vivek BPT 3 YearDocument26 pagesClinical Neurology Prepared By: Utkarsha and Vivek BPT 3 YearVivekChandaNo ratings yet
- MDCT and MRI Evaluation of Cervical Spine Trauma: Pictorial ReviewDocument9 pagesMDCT and MRI Evaluation of Cervical Spine Trauma: Pictorial ReviewcalinmariusNo ratings yet
- Fractura Columnae VertebralisDocument4 pagesFractura Columnae VertebralisTheo DapamedeNo ratings yet
- 7 - Spinal-InjuriesDocument40 pages7 - Spinal-Injuriesraed faisalNo ratings yet
- Spinal Cord InjuryDocument25 pagesSpinal Cord InjurySolsona Natl HS Maananteng100% (2)
- Fracture of Neck of FemurDocument13 pagesFracture of Neck of FemurRosemarie AbelaNo ratings yet
- Applied Anatomy: Head and NeckDocument9 pagesApplied Anatomy: Head and NeckdivinaNo ratings yet
- Spine and Spinal Cord TraumaDocument29 pagesSpine and Spinal Cord Traumag3niu5No ratings yet
- Spinal Cord InjuryDocument9 pagesSpinal Cord Injuryta CNo ratings yet
- Fracture in Leg Tibia and FibulaDocument27 pagesFracture in Leg Tibia and Fibulachilsya shajiNo ratings yet
- Fracturas de La Porción Media Del Húmero en Adultos - UpToDateDocument37 pagesFracturas de La Porción Media Del Húmero en Adultos - UpToDateRogelio MoscosoNo ratings yet
- Fractures of The Cervical Spine: ReviewDocument7 pagesFractures of The Cervical Spine: ReviewMeri Fitria HandayaniNo ratings yet
- CNS PBL 2Document6 pagesCNS PBL 2Hugh JacobsNo ratings yet
- Adult Traumatic Brachial Plexus InjuriesDocument15 pagesAdult Traumatic Brachial Plexus Injuriesapi-241264935No ratings yet
- Broken Neck (Hangman's Fracture) : DescriptionDocument5 pagesBroken Neck (Hangman's Fracture) : DescriptionFatima RizwanNo ratings yet
- Injuries of Shoulder Girdle Clavicle Fracture Scapula FractureDocument31 pagesInjuries of Shoulder Girdle Clavicle Fracture Scapula FractureWinda LiraNo ratings yet
- Litrev SCHDocument7 pagesLitrev SCHdedyalkarni08No ratings yet
- Human Spinal Cord Picture C1 To S5 VertebraDocument3 pagesHuman Spinal Cord Picture C1 To S5 Vertebraajjju02No ratings yet
- Acute Traumatic Spinal Cord InjuryDocument21 pagesAcute Traumatic Spinal Cord InjuryAmada Angel VillanuevaNo ratings yet
- Spinal Cord Trauma Nerve RootsDocument14 pagesSpinal Cord Trauma Nerve RootsAlyssa Thea Ablang TeofiloNo ratings yet
- Spinal Fracture - WikipediaDocument20 pagesSpinal Fracture - WikipediaLOURTHU PACKIA SAVARIMUTHU. MNo ratings yet
- Spinal Cord Injury and CompressionDocument10 pagesSpinal Cord Injury and CompressionAdeputhNo ratings yet
- Cervical Spine InjuryDocument18 pagesCervical Spine InjuryGabriel KlemensNo ratings yet
- Shoulder PathologiesDocument33 pagesShoulder PathologiesjermaineNo ratings yet
- Ilmiah Radilogi Dr. YuyunDocument59 pagesIlmiah Radilogi Dr. YuyunMia Pradana NingtyasNo ratings yet
- Blue Writing Is What I Added To These Notes: RadiographyDocument46 pagesBlue Writing Is What I Added To These Notes: Radiographybjpalmer100% (2)
- Radiography of The Cervical Spine in Trauma. Authors Thad Jackson & Deborah Blades (2002)Document21 pagesRadiography of The Cervical Spine in Trauma. Authors Thad Jackson & Deborah Blades (2002)Sean R. SmithNo ratings yet
- Ortho Questions 1Document10 pagesOrtho Questions 1Kay BristolNo ratings yet
- Spinal Cord Injuries and SyndromeDocument18 pagesSpinal Cord Injuries and SyndromeKim Sunoo100% (1)
- C14 - Coloana Vertebrala Engleza 2Document109 pagesC14 - Coloana Vertebrala Engleza 2Andreea DanielaNo ratings yet
- Mri Evaluation of Shoulder Joint: Normal Anatomy & Pathological Finding A Pictorial Essay and ReviewDocument9 pagesMri Evaluation of Shoulder Joint: Normal Anatomy & Pathological Finding A Pictorial Essay and ReviewIqhe Harsono SyastrowinotoNo ratings yet
- Ultrasonography of the Lower Extremity: Sport-Related InjuriesFrom EverandUltrasonography of the Lower Extremity: Sport-Related InjuriesNo ratings yet
- Acromioclavicular Joint Injury, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAcromioclavicular Joint Injury, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Bed Side Teaching: Siska Sarwana 712015035 Dr. Rizal Daulay, SP - OT, MARSDocument20 pagesBed Side Teaching: Siska Sarwana 712015035 Dr. Rizal Daulay, SP - OT, MARSAde ZulfiahNo ratings yet
- OKU Referat Bedah PDFDocument469 pagesOKU Referat Bedah PDFAde ZulfiahNo ratings yet
- Outcome After Fixation of Ankle Fractures With An Injury To The SyndesmosisDocument8 pagesOutcome After Fixation of Ankle Fractures With An Injury To The SyndesmosisAde ZulfiahNo ratings yet
- Rhinitis, Food, AllergicDocument8 pagesRhinitis, Food, AllergicAde ZulfiahNo ratings yet
- Jurnal Uts CTDocument10 pagesJurnal Uts CTBUDINo ratings yet
- Anatomy State Exam1Document12 pagesAnatomy State Exam1Manisanthosh KumarNo ratings yet
- Maxillary Second PremolarsDocument44 pagesMaxillary Second PremolarsAmrit Singh Ahluwalia0% (1)
- Neck & Back PainDocument232 pagesNeck & Back PainAatif_Saif_80No ratings yet
- Cervical Spine X-Ray Interpretation OSCE GuideDocument6 pagesCervical Spine X-Ray Interpretation OSCE GuideBeeNo ratings yet
- Chapter 4 - Vertebral ColumnDocument30 pagesChapter 4 - Vertebral ColumnMahendran JayaramanNo ratings yet
- Cervical Spine InjuryDocument26 pagesCervical Spine InjuryNufit Haruna100% (1)
- VertebraeDocument28 pagesVertebraeGummaregula SattibabuNo ratings yet
- LWBK836 Ch111 p1194-1208Document15 pagesLWBK836 Ch111 p1194-1208metasoniko81No ratings yet
- Anatomy of Vertebral ColumnDocument59 pagesAnatomy of Vertebral ColumnRivan DwiutomoNo ratings yet
- FHP ResearchDocument61 pagesFHP ResearchPooja DaveNo ratings yet
- Test Methodology For Protection of Vehicle Occupants Against Anti-Vehicular Landmine EffectsDocument24 pagesTest Methodology For Protection of Vehicle Occupants Against Anti-Vehicular Landmine EffectssudhavelNo ratings yet
- Fracture NomenclatureDocument7 pagesFracture NomenclatureDhon de CastroNo ratings yet
- Imaging in Acute Torticollis NXPowerLiteDocument41 pagesImaging in Acute Torticollis NXPowerLiteOktaviana Sari DewiNo ratings yet
- Cross Sectional Anatomy of SpineDocument37 pagesCross Sectional Anatomy of SpineAvinash Gupta50% (2)
- Neurological Physiotherapy Evaluation Form 2 0Document82 pagesNeurological Physiotherapy Evaluation Form 2 0Eman SabryNo ratings yet
- Cerda Et Al - 2021Document17 pagesCerda Et Al - 2021Jose L CarballidoNo ratings yet
- Vol I - Oase, Articulatii, Ligamente Si Muschi PDFDocument454 pagesVol I - Oase, Articulatii, Ligamente Si Muschi PDFBianca Byby100% (1)
- Median (Third) Occipital CondyleDocument4 pagesMedian (Third) Occipital Condylespin_echoNo ratings yet
- Human Anatomy 7Th Edition Marieb Test Bank Full Chapter PDFDocument43 pagesHuman Anatomy 7Th Edition Marieb Test Bank Full Chapter PDFStevenAdkinsyjmd100% (11)
- Elective Cases2aDocument156 pagesElective Cases2aMerlin MariandariNo ratings yet
- Osteology BonesDocument48 pagesOsteology BonesÂhmęd ĐoolaNo ratings yet
- (DD13-14) Anatomic SciencesDocument861 pages(DD13-14) Anatomic SciencesIndu C. R100% (2)
- Yoga Anatomy Physiology by ChopraDocument34 pagesYoga Anatomy Physiology by Choprarjil Comp100% (1)
- 0443065640Document447 pages0443065640Helena Sopen-Luoma100% (5)
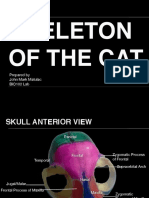
- Skeleton of The Cat: Prepared by John Mark Matulac BIO102 LabDocument27 pagesSkeleton of The Cat: Prepared by John Mark Matulac BIO102 LabJoachimNo ratings yet
- Spinal Neurosurgery 1St Edition James Harrop Editor Full Download ChapterDocument51 pagesSpinal Neurosurgery 1St Edition James Harrop Editor Full Download Chapterkristine.manning390100% (4)
- Cervical GoniometeryDocument39 pagesCervical GoniometerySimranjit KaurNo ratings yet
- Med SpinalDocument21 pagesMed SpinalDimas RenaldiNo ratings yet
- Which Parameters Are Relevant in Sagittal Balance Analysis of The Cervical Spine? A Literature ReviewDocument8 pagesWhich Parameters Are Relevant in Sagittal Balance Analysis of The Cervical Spine? A Literature ReviewMohsen AzarNo ratings yet