You might also like
- Neurology Notes - PassmedicineDocument71 pagesNeurology Notes - PassmedicineMohammad SalehNo ratings yet
- MRCP Commonly Tested Facts For Part1Document6 pagesMRCP Commonly Tested Facts For Part1Mohamed Amr SalamaNo ratings yet
- All Knowmedge Internal Medicine FlashcardDocument22 pagesAll Knowmedge Internal Medicine Flashcardrub100% (4)
- MKSAP NotesDocument31 pagesMKSAP NotesJared MasonNo ratings yet
- Short Answer Question SurgeryDocument9 pagesShort Answer Question SurgeryJohn M. Hemsworth100% (2)
- 0002 Rheumatology Notes 2015.... 49Document58 pages0002 Rheumatology Notes 2015.... 49Abdul QuyyumNo ratings yet
- 12 Weeks To Your Hottest Body EverDocument49 pages12 Weeks To Your Hottest Body EverSixp8ck100% (1)
- Acute Lymphoblastic LeukemiaDocument34 pagesAcute Lymphoblastic LeukemiamtyboyNo ratings yet
- Assessment of Systemic Lupus ErythematosusDocument13 pagesAssessment of Systemic Lupus ErythematosusBaso AgusofyangNo ratings yet
- Basic Pharmacology For Nurses 16th Edition Clayton Test BankDocument25 pagesBasic Pharmacology For Nurses 16th Edition Clayton Test BankKarenGonzalezinsz100% (57)
- Acute Lymphoblastic LeukemiaDocument19 pagesAcute Lymphoblastic LeukemiaNeng AyuRati50% (2)
- Presented By: Dr. Hirdesh Chawla Junior Resident IiiDocument79 pagesPresented By: Dr. Hirdesh Chawla Junior Resident IiiAzizan HannyNo ratings yet
- Necrotizing SialometaplasiaDocument33 pagesNecrotizing SialometaplasiaJessica GreenNo ratings yet
- Hyperbaric Oxygen Therapy, HBOT: Mohammad Guritno SURYOKUSUMODocument63 pagesHyperbaric Oxygen Therapy, HBOT: Mohammad Guritno SURYOKUSUMOAkbar AmirullahNo ratings yet
- PsorinumDocument55 pagesPsorinumHilery DorrianNo ratings yet
- Why Vegan PDFDocument12 pagesWhy Vegan PDFanimall0ver100% (1)
- SLE Concept MapDocument1 pageSLE Concept Mapadrienne cervantesNo ratings yet
- Lupus Nephritis1Document45 pagesLupus Nephritis1Lingga GumelarNo ratings yet
- DR - Nadrizal - Sle Dan RaDocument24 pagesDR - Nadrizal - Sle Dan RaPutri Sari SeptirianiNo ratings yet
- Portofolio SHDocument22 pagesPortofolio SHDini Jatiya AnggrainiNo ratings yet
- Systemic Lupus Erythematosus and Neuropsychiatric DiseaseDocument56 pagesSystemic Lupus Erythematosus and Neuropsychiatric DiseaseHerry HendrayadiNo ratings yet
- Systemic Lupus ErythematosusDocument3 pagesSystemic Lupus ErythematosusAlya Putri KhairaniNo ratings yet
- Systemic Lupus Erythematosus - An Overview: - Dr. Parvez KhanDocument68 pagesSystemic Lupus Erythematosus - An Overview: - Dr. Parvez KhanMohammad Sadiq AzamNo ratings yet
- LES Mar Cad OresDocument4 pagesLES Mar Cad OresAlberto StrusbergNo ratings yet
- Weekly Presentation and Discussion On Systemic Lupus Erythematosus (Sle)Document59 pagesWeekly Presentation and Discussion On Systemic Lupus Erythematosus (Sle)Dr AnilNo ratings yet
- Raynaud'S Phenomenon: Dr. Ajay Panwar Japi (May 2010)Document23 pagesRaynaud'S Phenomenon: Dr. Ajay Panwar Japi (May 2010)Ajay PanwarNo ratings yet
- Systemic Lupus Erythematosus (SLE)Document13 pagesSystemic Lupus Erythematosus (SLE)Kathrina IoannouNo ratings yet
- Farmakoterapi - SLEDocument28 pagesFarmakoterapi - SLEWidi Alya ZhafiraNo ratings yet
- 2014 - SLE LectureDocument96 pages2014 - SLE LectureDon CaprettoNo ratings yet
- Sle and Antiphoph, SclerodermaDocument63 pagesSle and Antiphoph, SclerodermaGermanyNo ratings yet
- Anesthesia For Systemic Lupus Erythematosus ReviewDocument12 pagesAnesthesia For Systemic Lupus Erythematosus ReviewAnonymous x75qV3lGNo ratings yet
- Lupus: Sigit Widyatmoko Fakultas Kedokteran UMSDocument52 pagesLupus: Sigit Widyatmoko Fakultas Kedokteran UMSAim AimmaNo ratings yet
- Neonatal Lupus ErythematosusDocument2 pagesNeonatal Lupus ErythematosusNatasha AmaldaNo ratings yet
- Efta Triastuti Study Program of Pharmacy Faculty of Medicine - Brawijaya UniversityDocument33 pagesEfta Triastuti Study Program of Pharmacy Faculty of Medicine - Brawijaya UniversityWidi Alya ZhafiraNo ratings yet
- Rheumatic Diseases and Vasculitis in ChildhoodDocument69 pagesRheumatic Diseases and Vasculitis in ChildhoodEslam HamadaNo ratings yet
- Systemic Lupus ErythematosusDocument6 pagesSystemic Lupus Erythematosuseka dharmaNo ratings yet
- SLE MedscapeDocument49 pagesSLE MedscapeAndino FadilNo ratings yet
- SleDocument66 pagesSlebhushan vichareNo ratings yet
- Antiphospholipidsyndrome 141019122948 Conversion Gate01Document50 pagesAntiphospholipidsyndrome 141019122948 Conversion Gate01asri khazaliNo ratings yet
- DR Is - Systemic Lupus ErythematosusDocument27 pagesDR Is - Systemic Lupus ErythematosusRizky SudarmaNo ratings yet
- Systemic Lupus Erythematosus: Harrison's ClubDocument60 pagesSystemic Lupus Erythematosus: Harrison's ClubOrchid Limoso LozanoNo ratings yet
- Systemic Lupus Erythematosus SLE: DefinitionDocument19 pagesSystemic Lupus Erythematosus SLE: DefinitionShimmering MoonNo ratings yet
- SleDocument33 pagesSleZaira HussainNo ratings yet
- Personal Notes Excpetional StuffDocument352 pagesPersonal Notes Excpetional StuffYagyeshNo ratings yet
- Myelodysplastic SyndromeDocument26 pagesMyelodysplastic SyndromeUmar'Farouq OniNo ratings yet
- Lupus ErythematosusDocument5 pagesLupus ErythematosusAditya DarmawanNo ratings yet
- Rheumatology Summary From AmbusDocument77 pagesRheumatology Summary From AmbusAlupoaie SilviuNo ratings yet
- Antiphospholipid Antibody Syndrome and PregnancyDocument17 pagesAntiphospholipid Antibody Syndrome and Pregnancybidan22No ratings yet
- Topic 8 Differential Diagnosis of FUO SCTD - Short.Document76 pagesTopic 8 Differential Diagnosis of FUO SCTD - Short.hhbhhNo ratings yet
- Acute Leukaemia Presentation 1Document20 pagesAcute Leukaemia Presentation 1Vaibhav KrishnaNo ratings yet
- Leukemia in ChildrenDocument44 pagesLeukemia in ChildrenSami ShouraNo ratings yet
- Int14 SLEDocument17 pagesInt14 SLEOsama AlhumisiNo ratings yet
- TEP EmergenciaDocument14 pagesTEP EmergenciaAntonio AlonsoNo ratings yet
- Histiocytic Disorders Diagnosis and Treatment: Resident Education Lecture SeriesDocument41 pagesHistiocytic Disorders Diagnosis and Treatment: Resident Education Lecture SeriesChetan SekhriNo ratings yet
- 2010 Childhood LeukaemiaDocument64 pages2010 Childhood LeukaemiaAnastasiafynnNo ratings yet
- Antiphospholipid SyndromeDocument32 pagesAntiphospholipid SyndromehziglamNo ratings yet
- Red Cell AplasiaDocument2 pagesRed Cell Aplasiaintrovoyz041No ratings yet
- Leukemia Pada AnakDocument33 pagesLeukemia Pada AnakandrianNo ratings yet
- Systemic Lupus ErythematosusDocument29 pagesSystemic Lupus ErythematosusNoreen PadillaNo ratings yet
- Sle NewestDocument70 pagesSle NewestTuhinaRajNo ratings yet
- Thesis Systemic Lupus ErythematosusDocument6 pagesThesis Systemic Lupus Erythematosuscaitlinwilsonsavannah100% (2)
- Arterial ThrombosisrheumroundsDocument49 pagesArterial ThrombosisrheumroundsBiniyam AsratNo ratings yet
- Acute LeukemiaDocument6 pagesAcute LeukemiaYolanda UriolNo ratings yet
- Almostadoctor Co Uk-LymphomaDocument14 pagesAlmostadoctor Co Uk-Lymphomaasif charsiNo ratings yet
- Systemic Lupus ErythematosusDocument10 pagesSystemic Lupus ErythematosuszkxxyyNo ratings yet
- Diagnosis and Management of Autoimmune Hepatitis: A Clinical GuideFrom EverandDiagnosis and Management of Autoimmune Hepatitis: A Clinical GuideMark W. RussoNo ratings yet
- The Most Dangerous Places and Travel Destinations in The WorldDocument5 pagesThe Most Dangerous Places and Travel Destinations in The WorldAhmedNo ratings yet
- Scorpion Toxins and Its ApplicationsDocument6 pagesScorpion Toxins and Its ApplicationschacanatorNo ratings yet
- Cordyceps 16mayvjDocument2 pagesCordyceps 16mayvjwarpansy15No ratings yet
- 01 The Living WorldDocument16 pages01 The Living Worldjocoge4337No ratings yet
- Tuberculosis: Nurul Najwa Binti Zulkifli (131855)Document18 pagesTuberculosis: Nurul Najwa Binti Zulkifli (131855)Nurul NajwaNo ratings yet
- Dental Management of AsthmaDocument8 pagesDental Management of AsthmaLorenzini GrantNo ratings yet
- Age of Exploration Scrapbook: By: Ben SteeleDocument12 pagesAge of Exploration Scrapbook: By: Ben Steeleapi-344972552No ratings yet
- ActinomycetesDocument15 pagesActinomycetesBenson100% (3)
- Sick PersonalityDocument4 pagesSick PersonalityAtul TyagiNo ratings yet
- HIV Infection and AIDS: Practice EssentialsDocument52 pagesHIV Infection and AIDS: Practice EssentialsRimaNo ratings yet
- Human Anatomy KROKDocument60 pagesHuman Anatomy KROKsushmitaNo ratings yet
- PURBANCHAL UNIVERSITY - ReportDocument29 pagesPURBANCHAL UNIVERSITY - ReportAsh-i ShNo ratings yet
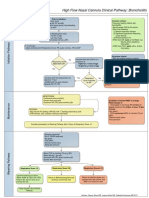
- High Flow Nasal Cannula Clinical Pathway: Bronchiolitis: Prior To Initiation: Inclusion CriteriaDocument1 pageHigh Flow Nasal Cannula Clinical Pathway: Bronchiolitis: Prior To Initiation: Inclusion Criteriad'Agung NugrohoNo ratings yet
- Mappimg Kamar 1 Dan 5Document4 pagesMappimg Kamar 1 Dan 5Satrya DitaNo ratings yet
- Bolo Vs PerfusiónDocument6 pagesBolo Vs Perfusión1cucu0No ratings yet
- Antenatal CareDocument29 pagesAntenatal Careعبدالكريم الاسدNo ratings yet
- Coronavirus (COVID-19) Records 26Document3 pagesCoronavirus (COVID-19) Records 26jmkenziehallNo ratings yet
- N7 by Novo - Methods of ContraceptionDocument34 pagesN7 by Novo - Methods of ContraceptionEllen Rose NovoNo ratings yet
- The All India Services (Med Att Rules) - Misc InstructionsDocument22 pagesThe All India Services (Med Att Rules) - Misc InstructionsJitendra Suraaj TripathiNo ratings yet
- Punjab Examination Commission 2019 5th Class Science Part A Objective Model PaperDocument4 pagesPunjab Examination Commission 2019 5th Class Science Part A Objective Model PaperTayyabah Shah100% (1)
- Is Stress Good For YouDocument3 pagesIs Stress Good For YoupavankumarmtNo ratings yet
- Chapter 1Document3 pagesChapter 1Anabelle SerranoNo ratings yet
- Hematology 2 Lesson 1Document9 pagesHematology 2 Lesson 1janNo ratings yet