You might also like
- Nelson Denny TestDocument2 pagesNelson Denny TestManuel Fermín Sánchez SánchezNo ratings yet
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- EN-Configurator - TSDZ2-mb.20beta1.ADocument14 pagesEN-Configurator - TSDZ2-mb.20beta1.AAlex GarridoNo ratings yet
- 4.krisis Hipertensi IMELS 15Document41 pages4.krisis Hipertensi IMELS 15putusanggraNo ratings yet
- Hypertension PresentationDocument97 pagesHypertension PresentationhawkansssNo ratings yet
- CIPD CH L 5 Org Dev and Reward PDFDocument80 pagesCIPD CH L 5 Org Dev and Reward PDFDrShabbir Khan50% (2)
- Jeppesen C-Map Professional Cm93 v3 Wf766Document5 pagesJeppesen C-Map Professional Cm93 v3 Wf766Ihwan Asrul100% (1)
- Krisis Hypertensi: Sigit Widyatmoko Fakultas KedokteranDocument85 pagesKrisis Hypertensi: Sigit Widyatmoko Fakultas KedokteranSeptian WidiantoNo ratings yet
- Hypertension OutlineDocument14 pagesHypertension OutlineMaria CayacoNo ratings yet
- Hypertensive CrisisDocument23 pagesHypertensive CrisisJayarani Ashok100% (1)
- Hypertensiveemergencies RullDocument60 pagesHypertensiveemergencies RullagustinaNo ratings yet
- HTN CDocument26 pagesHTN CharviliaNo ratings yet
- Hypertensive Emergency PDFDocument14 pagesHypertensive Emergency PDFOsiithaa CañaszNo ratings yet
- Hypertensive Crisis: Megat Mohd Azman Bin AdzmiDocument34 pagesHypertensive Crisis: Megat Mohd Azman Bin AdzmiMegat Mohd Azman AdzmiNo ratings yet
- Hypertensive Crisis: Philip Shayne and Catherine A. LynchDocument11 pagesHypertensive Crisis: Philip Shayne and Catherine A. LynchDong HkNo ratings yet
- Hypertensive CrisisDocument36 pagesHypertensive Crisisashwin choubeyNo ratings yet
- HYPERTENSION DR - Ridwan SPJPDocument43 pagesHYPERTENSION DR - Ridwan SPJPAmanda PutraNo ratings yet
- Hypertension: Hypertension Is One of The Most Common Worldwide Diseases Afflicting Humans. BecauseDocument8 pagesHypertension: Hypertension Is One of The Most Common Worldwide Diseases Afflicting Humans. BecauseKramojNo ratings yet
- HypertensionDocument46 pagesHypertensionUzma KhanNo ratings yet
- HYPERTENSIONDocument55 pagesHYPERTENSIONviennns100% (4)
- HypertensionDocument29 pagesHypertensionمبدر حامدNo ratings yet
- Hypertensive Vasular Disease For 2nd Yr PharmaDocument33 pagesHypertensive Vasular Disease For 2nd Yr PharmaYordanos GetnetNo ratings yet
- Hypertensive Encephalopathy: Presentation DDX Workup Treatment MedicationDocument8 pagesHypertensive Encephalopathy: Presentation DDX Workup Treatment MedicationMoh SuriyawalNo ratings yet
- Secondary Hypertension: S Ystolic-Diastolic Arterial HypetrtensionDocument9 pagesSecondary Hypertension: S Ystolic-Diastolic Arterial HypetrtensionvifawuduNo ratings yet
- Allan Lester VDocument6 pagesAllan Lester VA'Lester MedinaNo ratings yet
- Comprehensive Notes For Optometry - Systemic Diseases - 2023Document45 pagesComprehensive Notes For Optometry - Systemic Diseases - 2023Ramesh BabuNo ratings yet
- HypertensionDocument27 pagesHypertensionAnamika ChoudharyNo ratings yet
- HCVDDocument99 pagesHCVDMiguel CuevasNo ratings yet
- HYPERTENSIONDocument55 pagesHYPERTENSIONCut Putri RiskaNo ratings yet
- HypertensionDocument14 pagesHypertensionMr PresidentNo ratings yet
- Hypertension: Detection, Evaluation and Non-Pharmacologic InterventionDocument55 pagesHypertension: Detection, Evaluation and Non-Pharmacologic InterventionSyarif MaulanaNo ratings yet
- Hypertension Lecture NicvdDocument16 pagesHypertension Lecture NicvdNavojit ChowdhuryNo ratings yet
- Braunwald Lecture Series #2Document33 pagesBraunwald Lecture Series #2usfcards100% (2)
- Krisis Hypertensi: Sigit Widyatmoko Fakultas KedokteranDocument67 pagesKrisis Hypertensi: Sigit Widyatmoko Fakultas KedokteranLianSiahaanNo ratings yet
- Malignant Hypertension: Hypertensive EmergenciesDocument7 pagesMalignant Hypertension: Hypertensive EmergenciesAbdul QuyyumNo ratings yet
- 1 - HypertensionDocument35 pages1 - HypertensionLobna ElkilanyNo ratings yet
- Hypertension: Solomon E QuaysonDocument47 pagesHypertension: Solomon E QuaysonseadiabaNo ratings yet
- Dental Management in Medically Compromised Patients Hypertens IonDocument17 pagesDental Management in Medically Compromised Patients Hypertens Ionآلقہيہسہيہ مہجہآهہدNo ratings yet
- HTN Majdi FinalDocument87 pagesHTN Majdi FinalYaacoub ChahineNo ratings yet
- Management of The Patients With: Hypertensive CrisesDocument54 pagesManagement of The Patients With: Hypertensive CrisesДіна ШоріковаNo ratings yet
- HypertensionDocument12 pagesHypertensionDr. PARMINDER NAINNo ratings yet
- Hypertensive Emergencies: Sulaiman Usaid G. MBCHB V Facilatator: DR Jack TDocument44 pagesHypertensive Emergencies: Sulaiman Usaid G. MBCHB V Facilatator: DR Jack TUsaid SulaimanNo ratings yet
- Hypertensive CrisisDocument60 pagesHypertensive CrisisDzikrul Haq KarimullahNo ratings yet
- Hypertensive EmergencyDocument25 pagesHypertensive Emergencyzainab.mohammed.2307No ratings yet
- Krisis Hipertensi IMELSDocument43 pagesKrisis Hipertensi IMELSrinadi_aNo ratings yet
- HTN Crises For ResidentsDocument40 pagesHTN Crises For ResidentsImtiaz AhmadNo ratings yet
- Crisis HipertensivasDocument17 pagesCrisis HipertensivasJuan C. Moreno BarraganNo ratings yet
- Patofisiologi Krisis HipertensiDocument4 pagesPatofisiologi Krisis HipertensiAfriodita Ary PratiwiNo ratings yet
- Hypertensive Crisis2576 160125093408Document31 pagesHypertensive Crisis2576 160125093408Ceuro CeuroNo ratings yet
- Antihypertensive Drug LongDocument21 pagesAntihypertensive Drug Longa.muhsinNo ratings yet
- Chapter 33 HypertensionDocument5 pagesChapter 33 HypertensiongytmbiuiNo ratings yet
- Krisis HipertensiDocument12 pagesKrisis HipertensiDani NurseNo ratings yet
- Lec 3Document13 pagesLec 3fbbqbcht6yNo ratings yet
- Hypertensive Crises: Diagnosis and Management in The Emergency RoomDocument10 pagesHypertensive Crises: Diagnosis and Management in The Emergency RoomGede AdiNo ratings yet
- Essential Hypertension - StudentsDocument43 pagesEssential Hypertension - StudentsMohamoud MohamedNo ratings yet
- Awad ASDocument8 pagesAwad ASPedro VillamorNo ratings yet
- Pathophysiology: Cardiovascular System Dr. Maen DweikDocument38 pagesPathophysiology: Cardiovascular System Dr. Maen DweikshoibyNo ratings yet
- Cardiovascular Diseases 1Document13 pagesCardiovascular Diseases 1SRO oONo ratings yet
- Hypertensive Crisis PathoDocument4 pagesHypertensive Crisis PathoJanelle Dela CruzNo ratings yet
- HTN EmergenciesDocument7 pagesHTN EmergenciesBarry Tumpal Wouter NapitupuluNo ratings yet
- Chemical Pathology of HypertensionDocument37 pagesChemical Pathology of Hypertensionp6hccq6jd7No ratings yet
- CH 33 Key PointsDocument4 pagesCH 33 Key PointsKara Dawn MasonNo ratings yet
- Hypertensive Emergency: Beny Ghufron Dept. of Internal Medicine June 2011Document31 pagesHypertensive Emergency: Beny Ghufron Dept. of Internal Medicine June 2011Dendian Berlia JelitaNo ratings yet
- WHLP - Oct 5 9 - Ap 8Document10 pagesWHLP - Oct 5 9 - Ap 8rheyNo ratings yet
- Airspan ASMAX Product Brochure (QuantumWimax - Com)Document20 pagesAirspan ASMAX Product Brochure (QuantumWimax - Com)Ari Zoldan100% (1)
- ACDS Patch Testing To Propylene Glycol2.7.18Document20 pagesACDS Patch Testing To Propylene Glycol2.7.18Henry NguyenNo ratings yet
- CKM Advocates LLP SUITE 213, 2 Floor Marsabit PlazaDocument3 pagesCKM Advocates LLP SUITE 213, 2 Floor Marsabit PlazaMartha OumaNo ratings yet
- Piers Unit IVDocument36 pagesPiers Unit IVSuryaNo ratings yet
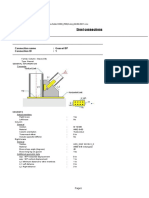
- Steel Connections: Detailed ReportDocument7 pagesSteel Connections: Detailed Reportgv Sathishkumar KumarNo ratings yet
- Chapter 02 Chemical Kinetics - March 2016Document84 pagesChapter 02 Chemical Kinetics - March 2016Ovinderjit SinghNo ratings yet
- Wayne Helix 1000Document15 pagesWayne Helix 1000Sanjeeb SinhaNo ratings yet
- 11 Student HandbookDocument12 pages11 Student HandbookMarianne RogersNo ratings yet
- C.TOUCH 2.0 USR Manual 1.0.6: Revision HistoryDocument21 pagesC.TOUCH 2.0 USR Manual 1.0.6: Revision HistoryNipun KumarNo ratings yet
- Cardiac ReportDocument71 pagesCardiac ReportManoj KumarNo ratings yet
- Davao Oriental State College of Science and Technology: SyllabusDocument7 pagesDavao Oriental State College of Science and Technology: SyllabusDaniel Jorolan Baldoz Jr.No ratings yet
- Bryant Oden Homework SongDocument4 pagesBryant Oden Homework Songehrcyltif100% (1)
- Huawei Emu: by Jefferson SimarmataDocument17 pagesHuawei Emu: by Jefferson SimarmataRZNo ratings yet
- MP Lab ManualDocument11 pagesMP Lab ManualRaj KumarNo ratings yet
- pt0 002 01Document28 pagespt0 002 01shilkee deviNo ratings yet
- Total Internal ReflectionDocument12 pagesTotal Internal ReflectionHarsh WardhanNo ratings yet
- Syllabus EnglishDocument24 pagesSyllabus EnglishmacjeromemanuelNo ratings yet
- Topic 7 Duties of The CitizensDocument16 pagesTopic 7 Duties of The CitizensMc Bryan CortezNo ratings yet
- Dried Mango and Mango Juice ProductionDocument78 pagesDried Mango and Mango Juice Productiontim mendozaNo ratings yet
- Guia Diy Employee ExperienceDocument45 pagesGuia Diy Employee ExperienceAnonymous Me42VYfQ100% (1)
- OLAYAO - Weekly Activity 2Document2 pagesOLAYAO - Weekly Activity 2Maki OlayaoNo ratings yet
- DLL Science-6 Q3 W6Document4 pagesDLL Science-6 Q3 W6juvelyn.aclaoNo ratings yet
- Soil WebquestDocument5 pagesSoil Webquestapi-264220291No ratings yet
- Cellonics Technology Seminar ReportDocument23 pagesCellonics Technology Seminar Reportnm gunasekharNo ratings yet
- Senior High School Electronic Class RecordDocument37 pagesSenior High School Electronic Class RecordSaiza BarrientosNo ratings yet