You might also like
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- Policy and Procedures For Hiring, PromotionsDocument2 pagesPolicy and Procedures For Hiring, PromotionsRazel Ann ElagioNo ratings yet
- Cyanotic Heart DiseaseDocument47 pagesCyanotic Heart Disease87-Saranya MNo ratings yet
- Lesson Plan Personality DisorderDocument7 pagesLesson Plan Personality DisorderRaj MeghwalNo ratings yet
- Congenital Heart DiseaseDocument55 pagesCongenital Heart DiseaseRaviNo ratings yet
- Congenital Heart DefectsDocument73 pagesCongenital Heart DefectsStaen KisNo ratings yet
- Pathophysiology Congenital Heart Disease-1Document54 pagesPathophysiology Congenital Heart Disease-1single_ladyNo ratings yet
- Decreased Pulmonary Blood Flow (CYANOTIC HEART DEFECTS)Document88 pagesDecreased Pulmonary Blood Flow (CYANOTIC HEART DEFECTS)leenaNo ratings yet
- Cyanotic Congenital Heart DiseaseDocument22 pagesCyanotic Congenital Heart DiseaseRaviNo ratings yet
- University of Saint Louis Tuguegarao City, Philippines: Maternal and Child Health NursingDocument69 pagesUniversity of Saint Louis Tuguegarao City, Philippines: Maternal and Child Health NursingErica Veluz LuyunNo ratings yet
- cvs2 CHDDocument27 pagescvs2 CHDIda WilonaNo ratings yet
- Penyakit Jantung KongenitalDocument30 pagesPenyakit Jantung KongenitalrintiikNo ratings yet
- 01 Cardiovascular IDocument72 pages01 Cardiovascular IcoriezaNo ratings yet
- ucu-CHDs 240114 230618Document68 pagesucu-CHDs 240114 230618BrianNo ratings yet
- Cardio-Respiratory Conditions: by DR Priscus MushiDocument73 pagesCardio-Respiratory Conditions: by DR Priscus MushiMusaNo ratings yet
- Cyanotic Heart LesionsDocument40 pagesCyanotic Heart LesionsRaison D'etreNo ratings yet
- Cyanotic Heart Disease: Dr.B.BalagobiDocument38 pagesCyanotic Heart Disease: Dr.B.BalagobiGomathi ShankarNo ratings yet
- CardiologyDocument43 pagesCardiologyhasanatiya41No ratings yet
- Congenital Heart Diseases: Charles University of Prague 2 Faculty of Medicine Filip KoubekDocument43 pagesCongenital Heart Diseases: Charles University of Prague 2 Faculty of Medicine Filip KoubekAdel HamzicNo ratings yet
- CME Cyanotic Heart DiseaseDocument38 pagesCME Cyanotic Heart DiseaseTan Zhi HongNo ratings yet
- Congenital Heart Defects: Module F Chapter Eleven Cardiac System Pages 348 - 359Document48 pagesCongenital Heart Defects: Module F Chapter Eleven Cardiac System Pages 348 - 359Sasikala MohanNo ratings yet
- Cyanotic Heart DiseaseDocument66 pagesCyanotic Heart DiseasePrasanth SankarNo ratings yet
- Paeds CardioDocument28 pagesPaeds CardioIman ZalzilahNo ratings yet
- Penyakit Jantung Bawaan II - 2Document30 pagesPenyakit Jantung Bawaan II - 2ahmad syauqieNo ratings yet
- #5 Neonatal Cardiac AnomaliesDocument93 pages#5 Neonatal Cardiac AnomaliesSittie Hania100% (2)
- Cardiovascular Diseases VSD Asd 2022 1Document16 pagesCardiovascular Diseases VSD Asd 2022 1Boyu GrtrNo ratings yet
- Tricuspid Atresia VivekDocument66 pagesTricuspid Atresia VivekIlham FatthurNo ratings yet
- Pda TofDocument56 pagesPda TofPritam PanigrahiNo ratings yet
- Cyanotic Congenital Heart DiseaseDocument50 pagesCyanotic Congenital Heart DiseaseSasi KumarNo ratings yet
- Cardio Vascular DisordersDocument62 pagesCardio Vascular DisordersUday Kumar100% (1)
- Congenital Heart DiseaseDocument77 pagesCongenital Heart DiseaseMalueth Angui100% (1)
- Adult CHD 2015Document42 pagesAdult CHD 2015Pshtiwan MahmoodNo ratings yet
- Odia Tetralogy of FallotDocument25 pagesOdia Tetralogy of Fallotvictorjonathan567No ratings yet
- Abnormal Heart Development 4-10-14 For BBDocument21 pagesAbnormal Heart Development 4-10-14 For BBroman7dbNo ratings yet
- Congenital Heart DiseaseDocument135 pagesCongenital Heart DiseaseMahmudahNo ratings yet
- Cardio HaikuDocument84 pagesCardio HaikugarifoNo ratings yet
- Cardio 2024Document42 pagesCardio 2024Salameh AtrashNo ratings yet
- Cardio My Opa ThiesDocument73 pagesCardio My Opa Thiesriyazadsumaiyajb2003No ratings yet
- CTSU Presentation PDADocument41 pagesCTSU Presentation PDAEdwin OkonNo ratings yet
- Congenital Heart DeseasesDocument54 pagesCongenital Heart DeseasesAntony100% (1)
- Congenital Heart Disease - Part IDocument95 pagesCongenital Heart Disease - Part IMeraol HusseinNo ratings yet
- 1.conginital Cardiac DefectsDocument39 pages1.conginital Cardiac DefectsJõsëph Jåy MîthNo ratings yet
- Congenital Cardiovascular AnomaliesDocument36 pagesCongenital Cardiovascular AnomaliesFauzi SatriaNo ratings yet
- Duct Dependent Lesions - PPSXDocument41 pagesDuct Dependent Lesions - PPSXSindujaNo ratings yet
- (I..) KMU Peads CardicDocument88 pages(I..) KMU Peads CardicMuhammadNo ratings yet
- Peds Shelf NotesDocument74 pagesPeds Shelf NotesRandy BornmannNo ratings yet
- Neonatology #30-41Document36 pagesNeonatology #30-41Daanish KhorasaniNo ratings yet
- Congenital Heart DiseasesDocument27 pagesCongenital Heart DiseasesJumar ValdezNo ratings yet
- Tetralogy of Fallot: DR Bhagirath S NDocument111 pagesTetralogy of Fallot: DR Bhagirath S NKunwar Sidharth SaurabhNo ratings yet
- Congenital Heart Disease: Faculty of Medicine University of BrawijayaDocument49 pagesCongenital Heart Disease: Faculty of Medicine University of BrawijayaShifa TifarinNo ratings yet
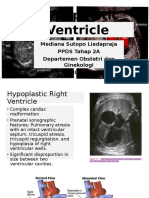
- Hypoplastic Ventricle. MEDIDocument21 pagesHypoplastic Ventricle. MEDIBenny Franclin SuripattyNo ratings yet
- Acyanotic Congenital Heart DiseaseDocument23 pagesAcyanotic Congenital Heart DiseasePernel Jose Alam MicuboNo ratings yet
- Congenital Heart Disease (CHD) : by Alireza PourtalebiDocument69 pagesCongenital Heart Disease (CHD) : by Alireza PourtalebiAswathy AswathyNo ratings yet
- Congenital Heart DiseasesDocument121 pagesCongenital Heart DiseasesJayvee V. De GuzmanNo ratings yet
- Pediatric Congenital Heart DiseaseDocument95 pagesPediatric Congenital Heart DiseaseShikya AbnasNo ratings yet
- Acyanotic Congenital Heart DiseaseDocument36 pagesAcyanotic Congenital Heart DiseaseRaviNo ratings yet
- 23 May 2011 Peerapat Thaisiam Yossavadee RuamcharoenDocument109 pages23 May 2011 Peerapat Thaisiam Yossavadee RuamcharoenRapid MedicineNo ratings yet
- Approach To Diagnosis of Congenital Heart DiseasesDocument85 pagesApproach To Diagnosis of Congenital Heart DiseasesNirav CHOVATIYANo ratings yet
- Congenital Disorder ASD VSDDocument50 pagesCongenital Disorder ASD VSDSachin DwivediNo ratings yet
- Congenital Heart Diseases, A Simple Guide to these Medical ConditionsFrom EverandCongenital Heart Diseases, A Simple Guide to these Medical ConditionsNo ratings yet
- RPLB NewDocument22 pagesRPLB NewMeta learnNo ratings yet
- Blood Stasis and What Does That MeanDocument2 pagesBlood Stasis and What Does That MeanCarl MacCordNo ratings yet
- Access To JusticeDocument9 pagesAccess To JusticeprimeNo ratings yet
- Reading Passage 1: IELTS Recent Actual Test With Answers Volume 1Document17 pagesReading Passage 1: IELTS Recent Actual Test With Answers Volume 1Amogha GadkarNo ratings yet
- Rudi Tampubolon - Risk Management ProcessDocument21 pagesRudi Tampubolon - Risk Management ProcessSeptian WisudaniNo ratings yet
- QTR-2 2023 Meeting Format Nov.23Document45 pagesQTR-2 2023 Meeting Format Nov.23skumar31397No ratings yet
- Dow Corning Corporation Material Safety Data SheetDocument9 pagesDow Corning Corporation Material Safety Data Sheetgazwang478No ratings yet
- Production & Downstream Processing of Baker's Best FriendDocument26 pagesProduction & Downstream Processing of Baker's Best FriendMelissaNo ratings yet
- Electrochemistry NotesDocument4 pagesElectrochemistry NotesAyush RorNo ratings yet
- Pressure Relief Valve, Poppet-Type, Direct-Acting: M28x1.5 - Q 50 L/min (13 GPM) - P 320 Bar (4600 PSI)Document2 pagesPressure Relief Valve, Poppet-Type, Direct-Acting: M28x1.5 - Q 50 L/min (13 GPM) - P 320 Bar (4600 PSI)Richam HamzeNo ratings yet
- Siklus Biogeokimia - Retensi NutrienDocument24 pagesSiklus Biogeokimia - Retensi NutrienPutri Nur Fadhilah YasharNo ratings yet
- Lab 5 - ReportDocument9 pagesLab 5 - ReportScarlet ErzaNo ratings yet
- Paraffin Wax Deposition: (The Challenges Associated and Mitigation Techniques, A Review)Document8 pagesParaffin Wax Deposition: (The Challenges Associated and Mitigation Techniques, A Review)Jit MukherheeNo ratings yet
- 150.66-RP4 YcalDocument92 pages150.66-RP4 YcalJosé RamosNo ratings yet
- Fleming Trio-E Promotional SheetDocument2 pagesFleming Trio-E Promotional SheetRed BarnNo ratings yet
- One Village One Product Movement in Laos: AbstractDocument5 pagesOne Village One Product Movement in Laos: Abstractoeleong19699685No ratings yet
- JECFA Carrageenan MonographDocument5 pagesJECFA Carrageenan MonographSurya SaputraNo ratings yet
- Metrel Mi 3290 Earth AnalyserDocument4 pagesMetrel Mi 3290 Earth AnalyserMarijan MustačNo ratings yet
- iSF EClassRecord - NewNormal AdviserDocument254 pagesiSF EClassRecord - NewNormal AdviserYanara Delarama DayapNo ratings yet
- Grammar Practice English Vi Second PartDocument8 pagesGrammar Practice English Vi Second PartBrando Olaya JuarezNo ratings yet
- 7-Day Indian Keto Diet Plan & Recipes For Weight LossDocument43 pages7-Day Indian Keto Diet Plan & Recipes For Weight LossachusanachuNo ratings yet
- Grandma StoriesDocument38 pagesGrandma StoriesSita Rani Devi DasiNo ratings yet
- Unit 1 Marks: 15 Introduction To Micro System and Smart SystemsDocument9 pagesUnit 1 Marks: 15 Introduction To Micro System and Smart SystemsSudarsh KNo ratings yet
- JSLHR Author InstructionsDocument14 pagesJSLHR Author InstructionsChanyanit CharoenpholNo ratings yet
- Ark of The Covenant Montessori Chamber of Learning PoblacionDocument3 pagesArk of The Covenant Montessori Chamber of Learning PoblacionMaiAce Sean Shawn SynneNo ratings yet
- Hitec 8888Z Atf C4 & To4 - TDSDocument2 pagesHitec 8888Z Atf C4 & To4 - TDSPranit More Arabian Petroleum LimitedNo ratings yet
- Mem CalcDocument6 pagesMem CalcQruisedNo ratings yet
- Karen Horney's Theories of PersonalityDocument8 pagesKaren Horney's Theories of PersonalityGeorge BaywongNo ratings yet