You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Learning Neuroimaging - 100 Essential CasesDocument239 pagesLearning Neuroimaging - 100 Essential CasesLaia Gasull100% (1)
- InfeksiDocument22 pagesInfeksiasepNo ratings yet
- Forehead Flap Reconstruction of Traumatic Nasal Tip AmputationDocument11 pagesForehead Flap Reconstruction of Traumatic Nasal Tip AmputationasepNo ratings yet
- Absen Apel 19 SepDocument1 pageAbsen Apel 19 SepasepNo ratings yet
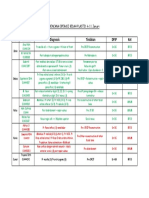
- Hari Identitas Diagnosis Tindakan DPJP Ket: Rencana Operasi Bedah Plastik 4-11 JanuariDocument1 pageHari Identitas Diagnosis Tindakan DPJP Ket: Rencana Operasi Bedah Plastik 4-11 JanuariasepNo ratings yet
- Bedah Plastik Selasa, 8 Januari 2019: Ruang Bed PJ DPJP Nama U MRS Diagnosis Status Plan Biaya LABDocument2 pagesBedah Plastik Selasa, 8 Januari 2019: Ruang Bed PJ DPJP Nama U MRS Diagnosis Status Plan Biaya LABasepNo ratings yet
- Surgical Approaches For Condylar Fractures Related To FacialDocument34 pagesSurgical Approaches For Condylar Fractures Related To FacialasepNo ratings yet
- Analisis StatistikDocument3 pagesAnalisis StatistikasepNo ratings yet
- Squamous CELL CARCINOMA Fix DNYDocument60 pagesSquamous CELL CARCINOMA Fix DNYasepNo ratings yet
- Burn Caused Brain InjuredDocument12 pagesBurn Caused Brain InjuredasepNo ratings yet
- Recent Publications On Myofunctional TherapyDocument5 pagesRecent Publications On Myofunctional TherapyasepNo ratings yet
- Antrian BangsalDocument1 pageAntrian BangsalasepNo ratings yet
- Dios 2005Document5 pagesDios 2005asepNo ratings yet
- Serialextraction 2Document6 pagesSerialextraction 2Zullia TaftyantiNo ratings yet
- Diagnosis & Treament: ShockDocument52 pagesDiagnosis & Treament: ShockasepNo ratings yet
- BionatorDocument1 pageBionatorasepNo ratings yet
- HOD Whitening RPT PDFDocument13 pagesHOD Whitening RPT PDFasepNo ratings yet
- En Bloc Mandibulectomy: Definition, Indications, Complications & ReferencesDocument10 pagesEn Bloc Mandibulectomy: Definition, Indications, Complications & Referencesasep100% (1)
- Technique To Manage The EnlargedDocument16 pagesTechnique To Manage The EnlargedasepNo ratings yet
- Processing ErrorsDocument19 pagesProcessing ErrorsasepNo ratings yet
- Analisis Sampel GpowerDocument1 pageAnalisis Sampel GpowerasepNo ratings yet
- Modern OrthodonticsDocument2 pagesModern OrthodonticsasepNo ratings yet
- Cerebellum, Thalamus, and HypothalamusDocument40 pagesCerebellum, Thalamus, and Hypothalamusasep100% (1)
- Modern DesignDocument50 pagesModern DesignasepNo ratings yet
- Oral Microorganism / Bacteria / Flora: EnvinronmentDocument3 pagesOral Microorganism / Bacteria / Flora: EnvinronmentasepNo ratings yet
- Apakah Bentuk Atom SEPERTI............. : V.Montgomery & R.Smith 1Document113 pagesApakah Bentuk Atom SEPERTI............. : V.Montgomery & R.Smith 1asepNo ratings yet
- Environmental Health in Healthcare FacilitiesDocument20 pagesEnvironmental Health in Healthcare FacilitiesasepNo ratings yet
- Processing ErrorsDocument19 pagesProcessing ErrorsasepNo ratings yet
- Anatomical LandmarkDocument12 pagesAnatomical LandmarkasepNo ratings yet
- Environmental Health in Healthcare FacilitiesDocument20 pagesEnvironmental Health in Healthcare FacilitiesasepNo ratings yet
- 2 Cytopathologic Changes in DiseaseDocument10 pages2 Cytopathologic Changes in DiseaseSandy GorricetaNo ratings yet
- 23rd PSCO ONCO 2019 Peshawar Agenda 1Document8 pages23rd PSCO ONCO 2019 Peshawar Agenda 1Mirza BaigNo ratings yet
- Cancer Stem CellsDocument7 pagesCancer Stem Cellskadir2613No ratings yet
- 【一般】Journal readingDocument28 pages【一般】Journal readingCY PNo ratings yet
- Understanding Male Genitourinary CancersDocument7 pagesUnderstanding Male Genitourinary CancersWoo Rin ParkNo ratings yet
- PMC Final Case StudyDocument41 pagesPMC Final Case StudydEEhY100% (1)
- Molinie 2018Document24 pagesMolinie 2018Veronica JanethNo ratings yet
- Cellulitis - Acute - NICE CKS PDFDocument40 pagesCellulitis - Acute - NICE CKS PDFDinu IuliaNo ratings yet
- Nevada Sagebrush Archives For 12012015Document14 pagesNevada Sagebrush Archives For 12012015The Nevada SagebrushNo ratings yet
- NeoplasiaDocument51 pagesNeoplasiaElstella Eguavoen Ehicheoya100% (1)
- Assessment of Sentinel Lymph Node Biopsy Vs Lymphadenectomy For Intermediate - and High-Grade Endometrial Cancer StagingDocument8 pagesAssessment of Sentinel Lymph Node Biopsy Vs Lymphadenectomy For Intermediate - and High-Grade Endometrial Cancer StagingEzequiel GonzalezNo ratings yet
- Challenging Neurological Manifestations in Large Cell Neuroendocrine Carcinoma Lcnec A Case Study of Extensive Intracranial and Intradural MetastasesDocument3 pagesChallenging Neurological Manifestations in Large Cell Neuroendocrine Carcinoma Lcnec A Case Study of Extensive Intracranial and Intradural MetastasesHerald Scholarly Open AccessNo ratings yet
- Cancer GeneticsDocument301 pagesCancer GeneticsNguyễn Tiến HồngNo ratings yet
- Improving Outcomes For Breast Cancer SurvivorsDocument280 pagesImproving Outcomes For Breast Cancer SurvivorsHồ Q. ThuậnNo ratings yet
- Overview of evaluating, diagnosing, and staging suspected lung cancerDocument197 pagesOverview of evaluating, diagnosing, and staging suspected lung cancerFernando HuertasNo ratings yet
- Cancer LaryncDocument35 pagesCancer LaryncSaya MenangNo ratings yet
- Introductory Q Bank (Pathology MCQ)Document9 pagesIntroductory Q Bank (Pathology MCQ)EZHIL N100% (1)
- MCQs NursingDocument3 pagesMCQs NursingNatalyaNo ratings yet
- NEOPLASIADocument35 pagesNEOPLASIAnnNo ratings yet
- LiposarcomaDocument9 pagesLiposarcomaFano Fahad TaihuttuNo ratings yet
- NRG-CC001 AA Protocol pv061015Document71 pagesNRG-CC001 AA Protocol pv061015markNo ratings yet
- Marjolin Ulcer POSTER (RSCM)Document1 pageMarjolin Ulcer POSTER (RSCM)Juli Jamnasi100% (1)
- Conjunctival MelanomaDocument11 pagesConjunctival MelanomaivanputrasNo ratings yet
- Breast Cancer ReportDocument8 pagesBreast Cancer ReportLevy Garcia SanchezNo ratings yet
- MicroCap Review Winter/Spring 2016Document96 pagesMicroCap Review Winter/Spring 2016Planet MicroCap Review MagazineNo ratings yet
- Utilizing Vitamin C To Treat Malignancies and Cancer: A Special Interview With Dr. Nathan GoodyearDocument42 pagesUtilizing Vitamin C To Treat Malignancies and Cancer: A Special Interview With Dr. Nathan GoodyearRocco LamponeNo ratings yet
- Jurnal NeoplasmaDocument10 pagesJurnal NeoplasmaFadhilah Asyifa DewantiNo ratings yet
- Mechanism of Lymph Node Metastasis in Prostate CancerDocument20 pagesMechanism of Lymph Node Metastasis in Prostate CancerAlexBritoNo ratings yet
- Johnson Jerry Alan Chinese Medical Qigong Therapy Vol 5-141-160Document20 pagesJohnson Jerry Alan Chinese Medical Qigong Therapy Vol 5-141-160toanbauNo ratings yet