You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- ISO 11064-12000 Ergonomic Design of Control Centres - Part 1 Principles For The Design of Control Centres by ISO TC 159SC 4WG 8Document6 pagesISO 11064-12000 Ergonomic Design of Control Centres - Part 1 Principles For The Design of Control Centres by ISO TC 159SC 4WG 8marcianocalvi4611100% (2)
- 28 ESL Discussion Topics Adult StudentsDocument14 pages28 ESL Discussion Topics Adult StudentsniallNo ratings yet
- Unit 3 DiathermyDocument63 pagesUnit 3 DiathermyAan Ika SugathotNo ratings yet
- Preliminary Voters ListDocument86 pagesPreliminary Voters Listمحمد منيب عبادNo ratings yet
- Refrensi Trauma KemihDocument1 pageRefrensi Trauma KemihMoch. Ivan KurniawanNo ratings yet
- BIO Chem Physio D I S E A S EDocument4 pagesBIO Chem Physio D I S E A S EMoch. Ivan KurniawanNo ratings yet
- Refrensi Trauma KemihDocument1 pageRefrensi Trauma KemihMoch. Ivan KurniawanNo ratings yet
- 3Document6 pages3Moch. Ivan KurniawanNo ratings yet
- Seven JumpDocument22 pagesSeven JumpMoch. Ivan KurniawanNo ratings yet
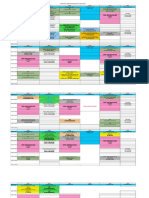
- Jadwal Blok THT Mata 2017 (1) Edit 1Document4 pagesJadwal Blok THT Mata 2017 (1) Edit 1Moch. Ivan KurniawanNo ratings yet
- Blepharitis 4Document2 pagesBlepharitis 4Moch. Ivan KurniawanNo ratings yet
- Jadwal Blok Tropmed Sem 7 FK UHT 2017-2018Document5 pagesJadwal Blok Tropmed Sem 7 FK UHT 2017-2018Moch. Ivan KurniawanNo ratings yet
- Journal Reading KulitDocument6 pagesJournal Reading KulitsintamirosmalindaNo ratings yet
- Ocular Toxoplasmosis - An Update and Review of The LiteratureDocument6 pagesOcular Toxoplasmosis - An Update and Review of The LiteratureMoch. Ivan KurniawanNo ratings yet
- Conjugata VeraDocument21 pagesConjugata VeraMoch. Ivan KurniawanNo ratings yet
- CV Old NicDocument4 pagesCV Old NicTensonNo ratings yet
- Accounting For A Service CompanyDocument9 pagesAccounting For A Service CompanyAnnie RapanutNo ratings yet
- Corporate Profile of Multimode GroupDocument6 pagesCorporate Profile of Multimode GroupShaheen RahmanNo ratings yet
- Wa200-8 Venss06304 1904 PDFDocument24 pagesWa200-8 Venss06304 1904 PDFOktiano BudiNo ratings yet
- SmoothWall Express 2.0 Quick-Start GuideDocument6 pagesSmoothWall Express 2.0 Quick-Start Guideinfobits100% (1)
- A Control Method For Power-Assist Devices Using A BLDC Motor For Manual WheelchairsDocument7 pagesA Control Method For Power-Assist Devices Using A BLDC Motor For Manual WheelchairsAhmed ShoeebNo ratings yet
- MELASMA (Ardy, Kintan, Fransisca)Document20 pagesMELASMA (Ardy, Kintan, Fransisca)Andi Firman MubarakNo ratings yet
- STS Reviewer FinalsDocument33 pagesSTS Reviewer FinalsLeiNo ratings yet
- Buy Wholesale China Popular Outdoor Football Boot For Teenagers Casual High Quality Soccer Shoes FG Ag Graffiti Style & FootballDocument1 pageBuy Wholesale China Popular Outdoor Football Boot For Teenagers Casual High Quality Soccer Shoes FG Ag Graffiti Style & Footballjcdc9chh8dNo ratings yet
- Auburn Bsci ThesisDocument5 pagesAuburn Bsci Thesisafksaplhfowdff100% (1)
- L&T Motor CatalogDocument24 pagesL&T Motor CatalogSanjeev DhariwalNo ratings yet
- Probecom 11.3M Antenna System Datasheet 2Document2 pagesProbecom 11.3M Antenna System Datasheet 2Hugo MateoNo ratings yet
- Lahainaluna High School Cafeteria: Lahaina, Maui, HawaiiDocument42 pagesLahainaluna High School Cafeteria: Lahaina, Maui, HawaiiKeerthy MoniNo ratings yet
- MSS SP 69pdfDocument18 pagesMSS SP 69pdfLaura CaballeroNo ratings yet
- Luyện nghe Tiếng Anh có đáp án: I/ Listen and complete the textDocument3 pagesLuyện nghe Tiếng Anh có đáp án: I/ Listen and complete the textVN LenaNo ratings yet
- In Other Words RE Increased by P250,000 (Income Less Dividends)Document6 pagesIn Other Words RE Increased by P250,000 (Income Less Dividends)Agatha de CastroNo ratings yet
- Haldex Valve Catalog: Quality Parts For Vehicles at Any Life StageDocument108 pagesHaldex Valve Catalog: Quality Parts For Vehicles at Any Life Stagehoussem houssemNo ratings yet
- Audit Committee and Corporate Governance: CA Pragnesh Kanabar Sir's The Audit Academy-CA Final AuditDocument17 pagesAudit Committee and Corporate Governance: CA Pragnesh Kanabar Sir's The Audit Academy-CA Final AuditPULKIT MURARKANo ratings yet
- Maryam Ejaz Sec-A Marketing Assignment (CHP #15)Document3 pagesMaryam Ejaz Sec-A Marketing Assignment (CHP #15)MaryamNo ratings yet
- Daewoo SJ-210H DSJ-6000LHMDocument44 pagesDaewoo SJ-210H DSJ-6000LHMMarco Antonio100% (5)
- Sorting Algorithms in Fortran: Dr. Ugur GUVENDocument10 pagesSorting Algorithms in Fortran: Dr. Ugur GUVENDHWANIT MISENo ratings yet
- Cell Structure, Cellular Respiration, PhotosynthesisDocument14 pagesCell Structure, Cellular Respiration, PhotosynthesisAmr NasserNo ratings yet
- (IGC 2024) 2nd Circular - 0630Document43 pages(IGC 2024) 2nd Circular - 0630VictoriaNo ratings yet
- Grade 7 First Quarter ExamDocument3 pagesGrade 7 First Quarter ExamBILLY JOE ARELLANONo ratings yet
- T10 - PointersDocument3 pagesT10 - PointersGlory of Billy's Empire Jorton KnightNo ratings yet
- Introductions and Basic Personal Information (In/Formal Communication)Document6 pagesIntroductions and Basic Personal Information (In/Formal Communication)juan morenoNo ratings yet
- Pe8 Mod5Document16 pagesPe8 Mod5Cryzel MuniNo ratings yet