You might also like
- Establishing Positive Relationships: Christine Foster, MA, LLPC, NCCDocument18 pagesEstablishing Positive Relationships: Christine Foster, MA, LLPC, NCCGr3y D3ngu3100% (1)
- Osprey, Men-At-Arms #039 The British Army in North America 1775-1783 (1998) (-) OCR 8.12Document49 pagesOsprey, Men-At-Arms #039 The British Army in North America 1775-1783 (1998) (-) OCR 8.12mancini100% (13)
- Module 1 2nd Quarter Per - Devt.Document15 pagesModule 1 2nd Quarter Per - Devt.Raiza Cabrera100% (1)
- Behavioural CommunicationDocument13 pagesBehavioural Communicationk_09100% (2)
- Chapter 3 Self AwarenessDocument34 pagesChapter 3 Self AwarenessNAASC Co.No ratings yet
- Concrete Masonry - Free Standing WallsDocument42 pagesConcrete Masonry - Free Standing WallsDaniel Liew100% (7)
- Estros Cycle in DogsDocument3 pagesEstros Cycle in DogsnessimmounirNo ratings yet
- VisArt10E SampleEbookDocument76 pagesVisArt10E SampleEbookFuture Managers Pty Ltd83% (6)
- A. Cultural Factors/ethnicity Such As Regard To Elders, Perception of HealthDocument6 pagesA. Cultural Factors/ethnicity Such As Regard To Elders, Perception of Healthlouie john abilaNo ratings yet
- Communication Skills With ElderlyDocument44 pagesCommunication Skills With ElderlyShereen Mohamed Soliman HammoudaNo ratings yet
- US Navy Course NAVEDTRA 14347 - Electronics Technician SupervisorDocument180 pagesUS Navy Course NAVEDTRA 14347 - Electronics Technician SupervisorGeorgesNo ratings yet
- Askeland Science and Engineering 7e ISM Chapter 04Document20 pagesAskeland Science and Engineering 7e ISM Chapter 04Ian Gabriel Cañas FernándezNo ratings yet
- Class 10 Life ProcessDocument11 pagesClass 10 Life ProcessShubham Tiwari100% (2)
- Talk with Confidence: A Comprehensive Guide to Effortless Communication with Anyone, Anytime, About AnythingFrom EverandTalk with Confidence: A Comprehensive Guide to Effortless Communication with Anyone, Anytime, About AnythingNo ratings yet
- Lesson Plan in Oral COmmunicationDocument4 pagesLesson Plan in Oral COmmunicationCarla CacharoNo ratings yet
- Marketing Plan For Madge Café: Caro, Marie Joy Casiple, Koleen Estebal, Honey Faye Longno, JosieDocument15 pagesMarketing Plan For Madge Café: Caro, Marie Joy Casiple, Koleen Estebal, Honey Faye Longno, JosieJoyNo ratings yet
- Barriers To Effective CommunicationDocument74 pagesBarriers To Effective CommunicationShiarica Mae NeriNo ratings yet
- V2.0.1 Windows Server and SQL Server Migration Audit ChecklistDocument27 pagesV2.0.1 Windows Server and SQL Server Migration Audit ChecklistFarisuddinFNo ratings yet
- Barriers To CommunicationDocument50 pagesBarriers To CommunicationachsurajNo ratings yet
- 6 - Communicating With Older AdultsDocument43 pages6 - Communicating With Older Adultsalishakr272No ratings yet
- Product Catalogue: Atlas Copco Ground Engineering ProductsDocument40 pagesProduct Catalogue: Atlas Copco Ground Engineering ProductshamidNo ratings yet
- Self-Learning Module: Valencia Colleges Inc. Hagkol, Valencia City Bukidnon 8709 PhilippinesDocument6 pagesSelf-Learning Module: Valencia Colleges Inc. Hagkol, Valencia City Bukidnon 8709 PhilippinesCarla Cacharo100% (2)
- Management Communication SlidesDocument62 pagesManagement Communication SlidesArie Bob100% (1)
- Module 5 Chapter 2: Communication: Communication: Verbal and NonverbalDocument7 pagesModule 5 Chapter 2: Communication: Communication: Verbal and Nonverbalgeni2009No ratings yet
- Culture, Health & Lifestyle Study Gude Chapter 2Document11 pagesCulture, Health & Lifestyle Study Gude Chapter 2JohnnyNguyenNo ratings yet
- Communication StylesDocument9 pagesCommunication StylesTaif SalimNo ratings yet
- 19.1 Psychosocial AspectDocument49 pages19.1 Psychosocial Aspectsushma shresthaNo ratings yet
- Week 2 - Barriers To CommunicationDocument29 pagesWeek 2 - Barriers To CommunicationMotlatsi JosephNo ratings yet
- 2 Types of Speech StyleDocument22 pages2 Types of Speech StyleJhay B. MagtibayNo ratings yet
- 6 Communication BarriersDocument42 pages6 Communication BarriersjiaNo ratings yet
- Unit 1 MBA Barriers To Communication NewDocument32 pagesUnit 1 MBA Barriers To Communication Newusless018No ratings yet
- Unit 3 - Creation of Healthy and Caring Relationships: A Scientific Approach To Health AEC 26Document23 pagesUnit 3 - Creation of Healthy and Caring Relationships: A Scientific Approach To Health AEC 26akash DongeNo ratings yet
- Communications and The Caregiving ProcessDocument6 pagesCommunications and The Caregiving ProcessMona DoriaNo ratings yet
- 25889newwwww Barrier To Communication 2Document31 pages25889newwwww Barrier To Communication 2SEHAR NadeeMNo ratings yet
- Communication Skills PDFDocument34 pagesCommunication Skills PDFManishNo ratings yet
- NCM CommunicationDocument7 pagesNCM Communicationprincessfarah hussinNo ratings yet
- Communication 2Document44 pagesCommunication 2Alih KathlyannNo ratings yet
- Basic Concepts of CommunicationDocument29 pagesBasic Concepts of CommunicationervinasetianingsihNo ratings yet
- L05 Unit 1 Barriers To CommunicationDocument30 pagesL05 Unit 1 Barriers To CommunicationShivam GuptaNo ratings yet
- NoiseDocument28 pagesNoiseeleendaNo ratings yet
- PD 22-Communication With Different Population GroupsDocument36 pagesPD 22-Communication With Different Population GroupsRZ NgNo ratings yet
- PD 22-Communication With Different Population GroupsDocument36 pagesPD 22-Communication With Different Population GroupsRZ NgNo ratings yet
- Stranger & Prediction Levels of CommunicationDocument28 pagesStranger & Prediction Levels of CommunicationSyed AhmadNo ratings yet
- Business Communication Iv Mba 2011 Batch: Second CAF AssignmentDocument9 pagesBusiness Communication Iv Mba 2011 Batch: Second CAF AssignmentPrerna ChopraNo ratings yet
- Barriers For Effective CommunicationDocument19 pagesBarriers For Effective CommunicationInduja TrNo ratings yet
- Communication Skills (RIU) Week-1 2-1Document49 pagesCommunication Skills (RIU) Week-1 2-1Muhammad TahirNo ratings yet
- CommunicationDocument44 pagesCommunicationivernjayNo ratings yet
- Welcome TO,: Barriers of CommunicationDocument12 pagesWelcome TO,: Barriers of CommunicationShraddhanjali SahooNo ratings yet
- 12 - Multiculturalism and EthicsDocument14 pages12 - Multiculturalism and EthicsBriannaNo ratings yet
- Importance of Body Language in Communication: Jennifer Beall, Pharmd, Bcps Jwbeall@Samford - Edu June 9, 2019Document44 pagesImportance of Body Language in Communication: Jennifer Beall, Pharmd, Bcps Jwbeall@Samford - Edu June 9, 2019HassanNo ratings yet
- Understanding Healthy Relationships PDFDocument10 pagesUnderstanding Healthy Relationships PDFBeatriz García MayordomoNo ratings yet
- Barrirs For CommunicationDocument35 pagesBarrirs For CommunicationShivu Yati100% (1)
- SFH Mod 3Document13 pagesSFH Mod 3goutami Sunthankar100% (1)
- 5 Communication, Culture, GenderDocument23 pages5 Communication, Culture, GenderSunaina arshadNo ratings yet
- Communication BarriersDocument40 pagesCommunication BarriersCarl Andrie MontefalcoNo ratings yet
- Nurses PledgeDocument46 pagesNurses PledgeJohn Dubik100% (1)
- Lec4 Barriers in Effective CommunicationDocument24 pagesLec4 Barriers in Effective CommunicationAmna MazharNo ratings yet
- Therapeutic Nurse - Patient RelationshipDocument53 pagesTherapeutic Nurse - Patient Relationshipسليمان العطويNo ratings yet
- Communicating Across CulturesDocument42 pagesCommunicating Across CulturesAaryav AnandNo ratings yet
- Communication BarriersDocument41 pagesCommunication BarriersMayankNo ratings yet
- Barriers To CommunicationDocument28 pagesBarriers To CommunicationVIVEKNo ratings yet
- Additional ReviewerDocument4 pagesAdditional ReviewerJamie Kayle N. LavitoriaNo ratings yet
- BCS Abnd SkillDocument34 pagesBCS Abnd Skillshri lakshmiNo ratings yet
- Purposive ComDocument54 pagesPurposive ComjulinaNo ratings yet
- Barriers To Cross-Cultural Counseling: Lack of Counselor Cultural Self-AwarenessDocument7 pagesBarriers To Cross-Cultural Counseling: Lack of Counselor Cultural Self-AwarenessNazri MusaNo ratings yet
- Chapter 6 Communication StyleDocument4 pagesChapter 6 Communication Stylegenevievegelinas7No ratings yet
- PDF Document 2Document24 pagesPDF Document 2Leira BalitaNo ratings yet
- Asian CultureDocument4 pagesAsian Cultureamitdce0178No ratings yet
- SEHH2045 2021 S2 L2 Communicating With Seniors UnlockedDocument55 pagesSEHH2045 2021 S2 L2 Communicating With Seniors UnlockedKikiNo ratings yet
- Level of ContextDocument5 pagesLevel of ContextLiz ViterboNo ratings yet
- Updated Ioer Membership FormDocument2 pagesUpdated Ioer Membership FormCarla CacharoNo ratings yet
- Bangcud National High SchoolDocument3 pagesBangcud National High SchoolCarla CacharoNo ratings yet
- Midterm Exam in OCDocument4 pagesMidterm Exam in OCCarla CacharoNo ratings yet
- EAAP QuizDocument2 pagesEAAP QuizCarla CacharoNo ratings yet
- Oral Communication in ContextDocument20 pagesOral Communication in ContextCarla CacharoNo ratings yet
- CathyDocument5 pagesCathyCarla CacharoNo ratings yet
- ICT Inventory Report S.Y. 2019-2020Document14 pagesICT Inventory Report S.Y. 2019-2020Carla CacharoNo ratings yet
- Cisco Ventura SchematicDocument242 pagesCisco Ventura SchematicpotatoNo ratings yet
- A Review On Gait Generation of The Biped Robot On Various TerrainsDocument43 pagesA Review On Gait Generation of The Biped Robot On Various Terrainsnarvan.m31No ratings yet
- Sony CCD-TR67 PDFDocument80 pagesSony CCD-TR67 PDFClemente GuerraNo ratings yet
- Module-1 ME 210 Metallurgy and Materials EngineeringDocument66 pagesModule-1 ME 210 Metallurgy and Materials EngineeringEDWIN K BABUNo ratings yet
- Daftar ECATALOG 2023 Yarindo For TP - 1 FebDocument6 pagesDaftar ECATALOG 2023 Yarindo For TP - 1 Febbayu setiawanNo ratings yet
- Conbehavior AnalysisDocument4 pagesConbehavior AnalysisKamil HasnainNo ratings yet
- Surgical Management of Dilocated Lens: Mohammad Ghoreishi, MDDocument15 pagesSurgical Management of Dilocated Lens: Mohammad Ghoreishi, MDwawan 88No ratings yet
- Binary and Hexadecimal Number SystemDocument4 pagesBinary and Hexadecimal Number Systemkaran007_m100% (3)
- Report of The Panel of Enquiry Into The Fire Incident at City Hall, Lagos, June, 1998Document27 pagesReport of The Panel of Enquiry Into The Fire Incident at City Hall, Lagos, June, 1998MrAyeDeeNo ratings yet
- Cetis D.D. Iso14001 Certificate 25082021 EngDocument2 pagesCetis D.D. Iso14001 Certificate 25082021 EngMonàm HadjiNo ratings yet
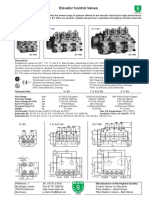
- Elevator Control Valves: EN ISO 9001Document6 pagesElevator Control Valves: EN ISO 9001Jibjab7No ratings yet
- Parent Record 74-75Document6 pagesParent Record 74-75Sujan BaralNo ratings yet
- Graphic Design and Lay Out MODULE 5Document24 pagesGraphic Design and Lay Out MODULE 5Shiela Fernando100% (1)
- Hydraulic Hammer Operators Manual: GH Series HammersDocument71 pagesHydraulic Hammer Operators Manual: GH Series HammersmarceloNo ratings yet
- The Bible, King James Version, Book 49: Ephesians by AnonymousDocument17 pagesThe Bible, King James Version, Book 49: Ephesians by AnonymousGutenberg.orgNo ratings yet
- Depo ProveraDocument3 pagesDepo ProveraNadine Abdel-GhafarNo ratings yet
- Angliiska Mova 5-Klas Karpuk 2013Document142 pagesAngliiska Mova 5-Klas Karpuk 2013Мовна Студія KIDSTREAMNo ratings yet
- Soal B-Inggris Try Out 1Document9 pagesSoal B-Inggris Try Out 1ukhti_ema100% (2)
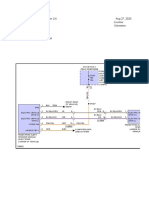
- 2020 Chrysler Voyager LXi 3.6LDocument134 pages2020 Chrysler Voyager LXi 3.6LGerardo MejiasNo ratings yet
- Maneurop® Reciprocating Compressors MT/MTZ: Application GuidelinesDocument42 pagesManeurop® Reciprocating Compressors MT/MTZ: Application GuidelinesIsidro MendozaNo ratings yet