You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Irr FinalDocument7 pagesIrr Finalapi-612103161No ratings yet
- JCRImpact Factor 2021Document526 pagesJCRImpact Factor 2021estuputriwirasNo ratings yet
- The Role of The Nurse in Health Promotion PDFDocument1 pageThe Role of The Nurse in Health Promotion PDFCie Ladd0% (1)
- Occuper's Liability (Textbook + Lecture Notes)Document28 pagesOccuper's Liability (Textbook + Lecture Notes)Malvika MahindraNo ratings yet
- Icd 10 Rajal Poli SarafDocument3 pagesIcd 10 Rajal Poli Sarafgrace efiliaNo ratings yet
- Cruz Marissa Resume CsusbDocument3 pagesCruz Marissa Resume Csusbapi-341233003No ratings yet
- Forthcoming Grand Chamber Case Vavricka and Others v. Czech RepublicDocument3 pagesForthcoming Grand Chamber Case Vavricka and Others v. Czech RepublicZiarul de GardăNo ratings yet
- Jerusalem SyndromeDocument5 pagesJerusalem Syndromele_papillon15No ratings yet
- NCP Shoulder DystociaDocument4 pagesNCP Shoulder DystociaTrishia CaroNo ratings yet
- Mpulungu Trust Summary ProfileDocument4 pagesMpulungu Trust Summary ProfileViktor Dmitri KanyozeNo ratings yet
- Part InequalyDocument30 pagesPart Inequalycoga81No ratings yet
- LEPROSY Part 2 - DR HannahDocument36 pagesLEPROSY Part 2 - DR HannahStase IKM FK UPHNo ratings yet
- Complementary and Alternative Health Care Client Bill of RightsDocument2 pagesComplementary and Alternative Health Care Client Bill of Rightsapi-31121402No ratings yet
- HIST311 Module 3Document3 pagesHIST311 Module 3Mey TysonNo ratings yet
- Practical Interpretation and Application of Exoc Rine Panc Rea Tic Tes Ting in Small AnimalsDocument20 pagesPractical Interpretation and Application of Exoc Rine Panc Rea Tic Tes Ting in Small Animalsl.fernandagonzalez97No ratings yet
- Performance Evaluation HeadnursingDocument3 pagesPerformance Evaluation HeadnursingBing58No ratings yet
- business-spotlight-2022-02-LEARNING TO COPEDocument5 pagesbusiness-spotlight-2022-02-LEARNING TO COPEvieilleecoleNo ratings yet
- ACLS (Notes) (Printable)Document2 pagesACLS (Notes) (Printable)mike_germain1172No ratings yet
- Introduction To FracturesDocument40 pagesIntroduction To FracturesAnisah Pangandag MapandiNo ratings yet
- MP5 - Option For The Bottom of The PyramidDocument25 pagesMP5 - Option For The Bottom of The Pyramid22ccg2f7d2No ratings yet
- IES College PlacementDocument10 pagesIES College PlacementpankajcpatelNo ratings yet
- Awareness of HIV/AIDS Among Grade 10 Students in Teofilo V. Fernandez National High SchoolDocument18 pagesAwareness of HIV/AIDS Among Grade 10 Students in Teofilo V. Fernandez National High SchoolChristine Jean CeredonNo ratings yet
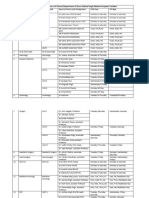
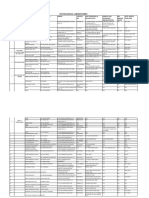
- OPD and OT Days of Doctors of Clinical Department of Guru Gobind Singh Medical HospitalDocument4 pagesOPD and OT Days of Doctors of Clinical Department of Guru Gobind Singh Medical HospitalBohar singh Brar BrarNo ratings yet
- Sustained Release Drug Delivery System Potential: The Pharma InnovationDocument13 pagesSustained Release Drug Delivery System Potential: The Pharma InnovationprinceamitNo ratings yet
- Pain Relief With Trigger Point Self-HelpDocument22 pagesPain Relief With Trigger Point Self-HelpMichelli Siqueira67% (9)
- Research IntroductionDocument18 pagesResearch IntroductionAngelica TebelinNo ratings yet
- Fneur 13 871187Document7 pagesFneur 13 871187Yery AparicioNo ratings yet
- Articles-Personality Process and Levels of DevelopmentDocument16 pagesArticles-Personality Process and Levels of DevelopmentbenhazanNo ratings yet
- High-Risk Pregnancy CareDocument34 pagesHigh-Risk Pregnancy CareShaufyqyn EzaniNo ratings yet
- District DataDocument242 pagesDistrict Dataayush.bullethealthcareNo ratings yet