
Stroke
Stroke
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- NTP MOP 6th Edition Pocket Guide PDFDocument96 pagesNTP MOP 6th Edition Pocket Guide PDFGJ LaderaNo ratings yet
- CV - Final22Document3 pagesCV - Final22ashishtritalNo ratings yet
- Platelet in DengueDocument5 pagesPlatelet in Denguekarina nilasariNo ratings yet
- Blood Donation: SMJK Kwang Hua, Klang Project Base Learning 2Document8 pagesBlood Donation: SMJK Kwang Hua, Klang Project Base Learning 2LOOK YU QI MoeNo ratings yet
- PDF Export 64cce1599ba62Document2 pagesPDF Export 64cce1599ba62joye24hoodaNo ratings yet
- Toothpaste SurveyDocument15 pagesToothpaste SurveyElaine Hicana CasilagNo ratings yet
- Personal and Professional Qualities of A Nurse PDFDocument1 pagePersonal and Professional Qualities of A Nurse PDFLeann Kate MartinezNo ratings yet
- Bulking Up: The Warfighter Nutrition GuideDocument10 pagesBulking Up: The Warfighter Nutrition GuideKim PetersenNo ratings yet
- Technical Englilsh I RP - ARGELIS - PEREZDocument38 pagesTechnical Englilsh I RP - ARGELIS - PEREZArgelis Lisset Prz HrnndzNo ratings yet
- Drug DiscoveryDocument28 pagesDrug DiscoveryAnki0391No ratings yet
- Van Asten ResumeDocument2 pagesVan Asten Resumeapi-499382707No ratings yet
- Def - Pemf LhymphoedemaDocument17 pagesDef - Pemf LhymphoedemaFisaudeNo ratings yet
- Article - 21 of CoiDocument18 pagesArticle - 21 of Coimohdarif.lawNo ratings yet
- H1 AntihistaminesDocument17 pagesH1 AntihistaminesRoppeNo ratings yet
- Dental Products MarketDocument19 pagesDental Products MarketVeronica BulatNo ratings yet
- Rasa Shastra PDFDocument6 pagesRasa Shastra PDFArya DeviNo ratings yet
- COSH Student Manual 062921Document195 pagesCOSH Student Manual 062921Sean SchneiderNo ratings yet
- 016 Procedure ScaffoldingDocument13 pages016 Procedure ScaffoldingHSE CERINo ratings yet
- Analisis Sistem Penyelenggaraan Rekam Medis Di Unit Rekam Medis Puskesmas Kota Wilayah Utara Kota KediriDocument9 pagesAnalisis Sistem Penyelenggaraan Rekam Medis Di Unit Rekam Medis Puskesmas Kota Wilayah Utara Kota Kedirikiki naniNo ratings yet
- Illicit Drug Use, Alcohol Abuse, and Internet Deviance (Sociology)Document30 pagesIllicit Drug Use, Alcohol Abuse, and Internet Deviance (Sociology)Amie Marie GeistmanNo ratings yet
- GANTT ChartDocument10 pagesGANTT ChartQuia Benjch UayanNo ratings yet
- Basic Electrical Safety Training (BEST)Document73 pagesBasic Electrical Safety Training (BEST)mark magpaleNo ratings yet
- Landguard A900: An Enzyme-Based Remediant For The Detoxification of Organophosphate Insecticides in Animal DipsDocument31 pagesLandguard A900: An Enzyme-Based Remediant For The Detoxification of Organophosphate Insecticides in Animal DipsStephen MooreNo ratings yet
- Module 4 - Applying Basic First AidDocument2 pagesModule 4 - Applying Basic First AidjessafesalazarNo ratings yet
- Parental Consent: Department of EducationDocument1 pageParental Consent: Department of EducationJovick BioNo ratings yet
- NDRRMC Update SitRep No. 22 Re Effects of Typhoon PEDRING (NESAT)Document37 pagesNDRRMC Update SitRep No. 22 Re Effects of Typhoon PEDRING (NESAT)Hiro Cerce Wilhelm ALDEN Abareta TonioNo ratings yet
- Srimanta Sankaradeva University of Health Sciences D. Pharm CourseDocument40 pagesSrimanta Sankaradeva University of Health Sciences D. Pharm CourseBeta BabuNo ratings yet
- NeuroimagingDocument47 pagesNeuroimagingKertiasihwayan100% (1)
- Tuhfatul BanatDocument98 pagesTuhfatul BanatAsma nauferNo ratings yet
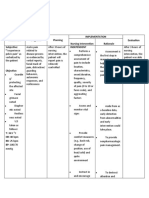
- Pelagio, Shiena Mae B. BSN Ii-A CASE: Cervical Cancer Implementation Nursing Intervention Rationale Evaluation Subjective: "I Experience IndependentDocument2 pagesPelagio, Shiena Mae B. BSN Ii-A CASE: Cervical Cancer Implementation Nursing Intervention Rationale Evaluation Subjective: "I Experience IndependentShiena Mae PelagioNo ratings yet




































































You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- NTP MOP 6th Edition Pocket Guide PDFDocument96 pagesNTP MOP 6th Edition Pocket Guide PDFGJ LaderaNo ratings yet
- CV - Final22Document3 pagesCV - Final22ashishtritalNo ratings yet
- Platelet in DengueDocument5 pagesPlatelet in Denguekarina nilasariNo ratings yet
- Blood Donation: SMJK Kwang Hua, Klang Project Base Learning 2Document8 pagesBlood Donation: SMJK Kwang Hua, Klang Project Base Learning 2LOOK YU QI MoeNo ratings yet
- PDF Export 64cce1599ba62Document2 pagesPDF Export 64cce1599ba62joye24hoodaNo ratings yet
- Toothpaste SurveyDocument15 pagesToothpaste SurveyElaine Hicana CasilagNo ratings yet
- Personal and Professional Qualities of A Nurse PDFDocument1 pagePersonal and Professional Qualities of A Nurse PDFLeann Kate MartinezNo ratings yet
- Bulking Up: The Warfighter Nutrition GuideDocument10 pagesBulking Up: The Warfighter Nutrition GuideKim PetersenNo ratings yet
- Technical Englilsh I RP - ARGELIS - PEREZDocument38 pagesTechnical Englilsh I RP - ARGELIS - PEREZArgelis Lisset Prz HrnndzNo ratings yet
- Drug DiscoveryDocument28 pagesDrug DiscoveryAnki0391No ratings yet
- Van Asten ResumeDocument2 pagesVan Asten Resumeapi-499382707No ratings yet
- Def - Pemf LhymphoedemaDocument17 pagesDef - Pemf LhymphoedemaFisaudeNo ratings yet
- Article - 21 of CoiDocument18 pagesArticle - 21 of Coimohdarif.lawNo ratings yet
- H1 AntihistaminesDocument17 pagesH1 AntihistaminesRoppeNo ratings yet
- Dental Products MarketDocument19 pagesDental Products MarketVeronica BulatNo ratings yet
- Rasa Shastra PDFDocument6 pagesRasa Shastra PDFArya DeviNo ratings yet
- COSH Student Manual 062921Document195 pagesCOSH Student Manual 062921Sean SchneiderNo ratings yet
- 016 Procedure ScaffoldingDocument13 pages016 Procedure ScaffoldingHSE CERINo ratings yet
- Analisis Sistem Penyelenggaraan Rekam Medis Di Unit Rekam Medis Puskesmas Kota Wilayah Utara Kota KediriDocument9 pagesAnalisis Sistem Penyelenggaraan Rekam Medis Di Unit Rekam Medis Puskesmas Kota Wilayah Utara Kota Kedirikiki naniNo ratings yet
- Illicit Drug Use, Alcohol Abuse, and Internet Deviance (Sociology)Document30 pagesIllicit Drug Use, Alcohol Abuse, and Internet Deviance (Sociology)Amie Marie GeistmanNo ratings yet
- GANTT ChartDocument10 pagesGANTT ChartQuia Benjch UayanNo ratings yet
- Basic Electrical Safety Training (BEST)Document73 pagesBasic Electrical Safety Training (BEST)mark magpaleNo ratings yet
- Landguard A900: An Enzyme-Based Remediant For The Detoxification of Organophosphate Insecticides in Animal DipsDocument31 pagesLandguard A900: An Enzyme-Based Remediant For The Detoxification of Organophosphate Insecticides in Animal DipsStephen MooreNo ratings yet
- Module 4 - Applying Basic First AidDocument2 pagesModule 4 - Applying Basic First AidjessafesalazarNo ratings yet
- Parental Consent: Department of EducationDocument1 pageParental Consent: Department of EducationJovick BioNo ratings yet
- NDRRMC Update SitRep No. 22 Re Effects of Typhoon PEDRING (NESAT)Document37 pagesNDRRMC Update SitRep No. 22 Re Effects of Typhoon PEDRING (NESAT)Hiro Cerce Wilhelm ALDEN Abareta TonioNo ratings yet
- Srimanta Sankaradeva University of Health Sciences D. Pharm CourseDocument40 pagesSrimanta Sankaradeva University of Health Sciences D. Pharm CourseBeta BabuNo ratings yet
- NeuroimagingDocument47 pagesNeuroimagingKertiasihwayan100% (1)
- Tuhfatul BanatDocument98 pagesTuhfatul BanatAsma nauferNo ratings yet
- Pelagio, Shiena Mae B. BSN Ii-A CASE: Cervical Cancer Implementation Nursing Intervention Rationale Evaluation Subjective: "I Experience IndependentDocument2 pagesPelagio, Shiena Mae B. BSN Ii-A CASE: Cervical Cancer Implementation Nursing Intervention Rationale Evaluation Subjective: "I Experience IndependentShiena Mae PelagioNo ratings yet