You might also like
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- Nursing Acn-IiDocument80 pagesNursing Acn-IiMunawar100% (6)
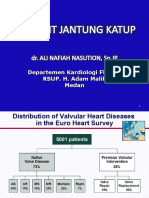
- K7 - Penyakit Jantung Katub-ANNDocument38 pagesK7 - Penyakit Jantung Katub-ANNXeniel AlastairNo ratings yet
- Valvular heart disease diagnosis and treatmentDocument38 pagesValvular heart disease diagnosis and treatmentDumora FatmaNo ratings yet
- Angelina A Joho MSC in Critical Care and TraumaDocument50 pagesAngelina A Joho MSC in Critical Care and TraumaZabron LuhendeNo ratings yet
- Department of Internal Medicine III Aortic Stenosis: - Rajkumar Subasaravanan Subgroup "12"Document51 pagesDepartment of Internal Medicine III Aortic Stenosis: - Rajkumar Subasaravanan Subgroup "12"Suba Saravanan 12No ratings yet
- Hypertrophic CardiomyopathyDocument32 pagesHypertrophic CardiomyopathyAbnet WondimuNo ratings yet
- Valvular Heart DiseaseDocument73 pagesValvular Heart Diseaseindia2puppy100% (4)
- Cardiac TamponadeDocument6 pagesCardiac TamponadeVicky XieNo ratings yet
- Valvular Heart Disease: Dr. Nigussie BerihunDocument43 pagesValvular Heart Disease: Dr. Nigussie Berihunsisay tigabuNo ratings yet
- Cardiovascular Function: Marquez, Spencer T. BSN Iii, Block Iv NCM 114, N134Document38 pagesCardiovascular Function: Marquez, Spencer T. BSN Iii, Block Iv NCM 114, N134hayascent hilarioNo ratings yet
- Valvular Heart Disease For Nurses by MR - Mihir.M.PatelDocument30 pagesValvular Heart Disease For Nurses by MR - Mihir.M.PatelMihir PatelNo ratings yet
- Cardiac Tamponade and ManagementDocument42 pagesCardiac Tamponade and Managementأم حمدNo ratings yet
- Aortic Regurgitation: Causes, Symptoms, and TreatmentDocument12 pagesAortic Regurgitation: Causes, Symptoms, and TreatmentSanjeet SahNo ratings yet
- Cardiac Tamponade: Pankaj Singh Rana Nurse Practitioner in Critical Care Swami Rama Himalayan UniversityDocument35 pagesCardiac Tamponade: Pankaj Singh Rana Nurse Practitioner in Critical Care Swami Rama Himalayan UniversityBarlonga Yhan YogaNo ratings yet
- Valvular Heart DiseaseDocument66 pagesValvular Heart DiseaseRita LakhaniNo ratings yet
- Mitral Stenosis Etiology and TreatmentDocument19 pagesMitral Stenosis Etiology and TreatmentAdi TrisnoNo ratings yet
- Valvular Heart Disease. KulDocument67 pagesValvular Heart Disease. KulDebyAntatifaniRitongaNo ratings yet
- PalpitationsDocument3 pagesPalpitationsJessica Febrina WuisanNo ratings yet
- Mitral Valve ProlapseDocument3 pagesMitral Valve ProlapseKristine CastilloNo ratings yet
- DR Ali Cardiology-MergedDocument684 pagesDR Ali Cardiology-MergedK PradhanNo ratings yet
- MITRAL STENOSIS AND AORTIC STENOSIS CAUSES, SYMPTOMS AND TREATMENTDocument6 pagesMITRAL STENOSIS AND AORTIC STENOSIS CAUSES, SYMPTOMS AND TREATMENTKobby AmoahNo ratings yet
- UMS20 Medical 20 Short 20 and 20 Long 20 Cases 20 Record 20 Second 20 EditiDocument132 pagesUMS20 Medical 20 Short 20 and 20 Long 20 Cases 20 Record 20 Second 20 EditiUchiha AnzarNo ratings yet
- Tuberculous Pericardial EffusionDocument6 pagesTuberculous Pericardial EffusionLink BuiNo ratings yet
- Mitral Stenosis Facts, Causes, Symptoms and TreatmentDocument16 pagesMitral Stenosis Facts, Causes, Symptoms and TreatmentAsrafur RahmanNo ratings yet
- Medical Surgery-2Document10 pagesMedical Surgery-2Wanjiku NderituNo ratings yet
- Acyanoticheartdiseases 180620040047 PDFDocument88 pagesAcyanoticheartdiseases 180620040047 PDFElijahNo ratings yet
- Acyanoticheartdiseases 180620040047 PDFDocument88 pagesAcyanoticheartdiseases 180620040047 PDFElijahNo ratings yet
- Acyanoticheartdiseases 180620040047 PDFDocument88 pagesAcyanoticheartdiseases 180620040047 PDFElijahNo ratings yet
- Cardiac Tamponade, Also Known As Pericardial Tamponade, Is AnDocument7 pagesCardiac Tamponade, Also Known As Pericardial Tamponade, Is AnSimran Josan100% (1)
- Aortic Regurgitation by DR DilmoDocument37 pagesAortic Regurgitation by DR Dilmosinan kNo ratings yet
- Rheumatic Heart DiseaseDocument47 pagesRheumatic Heart DiseaseGideon K. MutaiNo ratings yet
- Valvular Heart Disease 2Document46 pagesValvular Heart Disease 2Topea BogdanNo ratings yet
- DR Harris Hasan SPPD, SPJP (K) Departemen Kardiologi FK Usu MedanDocument46 pagesDR Harris Hasan SPPD, SPJP (K) Departemen Kardiologi FK Usu MedanAndi WiraNo ratings yet
- Cardio Vascular DisordersDocument62 pagesCardio Vascular DisordersUday Kumar100% (1)
- DR Harris Hasan SPPD, SPJP (K) Departemen Kardiologi FK Usu MedanDocument46 pagesDR Harris Hasan SPPD, SPJP (K) Departemen Kardiologi FK Usu MedanAziz DjohariNo ratings yet
- Casos Cardiológicos 1Document12 pagesCasos Cardiológicos 1Larissa SeabraNo ratings yet
- Pemicu 6 Eko Blok KGDDocument128 pagesPemicu 6 Eko Blok KGDEko SiswantoNo ratings yet
- Medicine: Aquired Valvular Heart DiseaseDocument3 pagesMedicine: Aquired Valvular Heart Diseaseapi-3829364No ratings yet
- ACFrOgC-pzE5RQJIbCELZhV0cdk6ioDNIaJcmCjwqiRF DrvgVB6DZwpe H0xKtsQ-azwWzcoEmilNTpD-bIlbSmB5BUuUaB1XyQtaHmg4Ko6DsOFWTXCUb6HV9ROfpC cuspVp0vX5MLV8nPIBCDocument67 pagesACFrOgC-pzE5RQJIbCELZhV0cdk6ioDNIaJcmCjwqiRF DrvgVB6DZwpe H0xKtsQ-azwWzcoEmilNTpD-bIlbSmB5BUuUaB1XyQtaHmg4Ko6DsOFWTXCUb6HV9ROfpC cuspVp0vX5MLV8nPIBCClaire GidoNo ratings yet
- Pathophysiology of Pericardial DiseaseDocument36 pagesPathophysiology of Pericardial DiseaseivaniNo ratings yet
- Types and Management of Valvular Heart DiseaseDocument60 pagesTypes and Management of Valvular Heart DiseaseIntan Kumalasari RambeNo ratings yet
- Valvular Heart Disease Nursing Care and DiagnosisDocument41 pagesValvular Heart Disease Nursing Care and DiagnosisVirendra Shekhawat100% (1)
- Cardiac FailureDocument63 pagesCardiac FailureNina OaipNo ratings yet
- Severe Calcified Mitral Stenosis and Atrial Fibrillation Lead to Ischemic StrokeDocument10 pagesSevere Calcified Mitral Stenosis and Atrial Fibrillation Lead to Ischemic StrokeDarawan MirzaNo ratings yet
- Heart FailureDocument39 pagesHeart FailureMuhammad AsifNo ratings yet
- SEMINARDocument31 pagesSEMINARDeveshNo ratings yet
- 3 - Valvular Heart DiseasesDocument31 pages3 - Valvular Heart DiseasesLobna ElkilanyNo ratings yet
- Congestive Heart Failure LathaDocument68 pagesCongestive Heart Failure LathaLatha GhanesanNo ratings yet
- Tiki Taka Notes Final PDFDocument104 pagesTiki Taka Notes Final PDFAditiSahak62No ratings yet
- Presented by Dona Mathew MSC (N) Govt - College of Nursing KottayamDocument221 pagesPresented by Dona Mathew MSC (N) Govt - College of Nursing KottayamSumathi GopinathNo ratings yet
- Congestive Heart FailureDocument6 pagesCongestive Heart Failureseigelystic100% (1)
- Cyanotic Congenital Heart DiseaseDocument58 pagesCyanotic Congenital Heart Diseasegolden37No ratings yet
- Ischemic Heart DiseaseDocument67 pagesIschemic Heart Diseasealfaz lakhani80% (5)
- Cardiology Notes by Wasim AhmadDocument28 pagesCardiology Notes by Wasim AhmadAshna moeenNo ratings yet
- Heart Failure: Classification, Risk Factors and Clinical FeaturesDocument48 pagesHeart Failure: Classification, Risk Factors and Clinical FeaturesMaria Cristina Sierralta SimonNo ratings yet
- CARDIAC FAILURE NewDocument60 pagesCARDIAC FAILURE NewJake MillerNo ratings yet
- Penyakit Jantung KatupDocument35 pagesPenyakit Jantung Katupdwi ariskaNo ratings yet
- The Heart-1Document30 pagesThe Heart-1Ebuka AniNo ratings yet
- Cyanotic Heart DiseaseDocument47 pagesCyanotic Heart Disease87-Saranya MNo ratings yet
- Isabela State University: Immunology (Bs Psych 2)Document4 pagesIsabela State University: Immunology (Bs Psych 2)Charlz ZipaganNo ratings yet
- Isabela State University: Immunology (Bs Psych 2)Document5 pagesIsabela State University: Immunology (Bs Psych 2)Charlz ZipaganNo ratings yet
- Isabela State University: Immunology (Bs Psych 2)Document5 pagesIsabela State University: Immunology (Bs Psych 2)Charlz ZipaganNo ratings yet
- Isabela State University City of Ilagan Campus: ImmunologyDocument18 pagesIsabela State University City of Ilagan Campus: ImmunologyCharlz ZipaganNo ratings yet
- Lec 1Document200 pagesLec 1Charlz ZipaganNo ratings yet
- Heart Anatomy and Function QuizDocument8 pagesHeart Anatomy and Function QuizCharlz ZipaganNo ratings yet
- Isabela State University City of Ilagan Campus: ImmunologyDocument18 pagesIsabela State University City of Ilagan Campus: ImmunologyCharlz ZipaganNo ratings yet
- Isabela State University: Immunology (Bs Psych 2)Document4 pagesIsabela State University: Immunology (Bs Psych 2)Charlz ZipaganNo ratings yet
- Controlling Communicable Diseases NCLEX ReviewDocument6 pagesControlling Communicable Diseases NCLEX ReviewCharlz ZipaganNo ratings yet
- Republic of The Philippines City of Ilagan Campus: Isabela State UniversityDocument2 pagesRepublic of The Philippines City of Ilagan Campus: Isabela State UniversityCharlz ZipaganNo ratings yet
- First QuizDocument6 pagesFirst QuizCharlz ZipaganNo ratings yet
- Interview Skills & Health History.: Charles Z. Ariola JR., MSN, Lpt. Instructor IIIDocument17 pagesInterview Skills & Health History.: Charles Z. Ariola JR., MSN, Lpt. Instructor IIICharlz ZipaganNo ratings yet
- Chest PhysiotherapyDocument51 pagesChest PhysiotherapyCharlz ZipaganNo ratings yet
- Isabela State University: Immunology (Bs Psych 2)Document8 pagesIsabela State University: Immunology (Bs Psych 2)Charlz ZipaganNo ratings yet
- First QuizDocument6 pagesFirst QuizCharlz ZipaganNo ratings yet
- MSN Discusses Activities of Daily Living and Factors Affecting ThemDocument11 pagesMSN Discusses Activities of Daily Living and Factors Affecting ThemCharlz ZipaganNo ratings yet
- Quiz 2Document5 pagesQuiz 2Charlz ZipaganNo ratings yet
- Gordon's Functional Health Patterns: A Case StudyDocument30 pagesGordon's Functional Health Patterns: A Case StudyCharlz ZipaganNo ratings yet
- Health History: Charles Z. Ariola JR., MSN, LPTDocument19 pagesHealth History: Charles Z. Ariola JR., MSN, LPTCharlz ZipaganNo ratings yet
- Interview Skills & Health History.: Charles Z. Ariola JR., MSN, Lpt. Instructor IIIDocument17 pagesInterview Skills & Health History.: Charles Z. Ariola JR., MSN, Lpt. Instructor IIICharlz ZipaganNo ratings yet
- Isabela State University City of Ilagan Campus: Care of The Clients With Endocrine and Metabolic DisorderDocument13 pagesIsabela State University City of Ilagan Campus: Care of The Clients With Endocrine and Metabolic DisorderCharlz ZipaganNo ratings yet
- MSN Discusses Activities of Daily Living and Factors Affecting ThemDocument11 pagesMSN Discusses Activities of Daily Living and Factors Affecting ThemCharlz ZipaganNo ratings yet
- HEALTH ASSESSMENT: A KEY COMPONENT OF NURSING PROCESSDocument83 pagesHEALTH ASSESSMENT: A KEY COMPONENT OF NURSING PROCESSCharlz ZipaganNo ratings yet
- MSN Discusses Activities of Daily Living and Factors Affecting ThemDocument11 pagesMSN Discusses Activities of Daily Living and Factors Affecting ThemCharlz ZipaganNo ratings yet
- Interview Skills & Health History.: Charles Z. Ariola JR., MSN, Lpt. Instructor IIIDocument17 pagesInterview Skills & Health History.: Charles Z. Ariola JR., MSN, Lpt. Instructor IIICharlz ZipaganNo ratings yet
- Isabela State University City of Ilagan Campus: Care of The Clients With Endocrine and Metabolic DisorderDocument29 pagesIsabela State University City of Ilagan Campus: Care of The Clients With Endocrine and Metabolic DisorderCharlz ZipaganNo ratings yet
- Isabela State University City of Ilagan Campus: Care of The Clients With Endocrine and Metabolic DisorderDocument15 pagesIsabela State University City of Ilagan Campus: Care of The Clients With Endocrine and Metabolic DisorderCharlz ZipaganNo ratings yet
- Isabela State University City of Ilagan Campus: Care of The Clients With Endocrine and Metabolic DisorderDocument13 pagesIsabela State University City of Ilagan Campus: Care of The Clients With Endocrine and Metabolic DisorderCharlz ZipaganNo ratings yet
- Isabela State University City of Ilagan Campus: Care of The Clients With Endocrine and Metabolic DisorderDocument29 pagesIsabela State University City of Ilagan Campus: Care of The Clients With Endocrine and Metabolic DisorderCharlz ZipaganNo ratings yet
- Isabela State University City of Ilagan Campus: Care of The Clients With Endocrine and Metabolic DisorderDocument15 pagesIsabela State University City of Ilagan Campus: Care of The Clients With Endocrine and Metabolic DisorderCharlz ZipaganNo ratings yet
- Kleinman & KleinmanDocument24 pagesKleinman & Kleinmanjigues100% (1)
- Pre Term Case OlieDocument10 pagesPre Term Case OlieKimsha ConcepcionNo ratings yet
- 1577un 2026-01Document79 pages1577un 2026-01ngovantienNo ratings yet
- Restoracion Del Organismo Humano 2 de 2Document56 pagesRestoracion Del Organismo Humano 2 de 2Eduardo UribeNo ratings yet
- AntacidsDocument2 pagesAntacidsMa Corazon MelecioNo ratings yet
- Cincinnati Police Use of Force PolicyDocument29 pagesCincinnati Police Use of Force PolicyCincinnatiEnquirerNo ratings yet
- Name of The Medicinal ProductDocument7 pagesName of The Medicinal Productddandan_2No ratings yet
- 8 Shaped WalkDocument1 page8 Shaped WalkAmy MyzaraNo ratings yet
- Probiotics For Preventing Urinary Tract Infections in Adults and Children - Schwenger, EM - 2015 - Cochrane LibraryDocument21 pagesProbiotics For Preventing Urinary Tract Infections in Adults and Children - Schwenger, EM - 2015 - Cochrane LibraryMixcy MabatidNo ratings yet
- Solution Manual For An Integrated Approach To Health Sciences Anatomy and Physiology Math Chemistry and Medical Microbiology 2nd EditionDocument4 pagesSolution Manual For An Integrated Approach To Health Sciences Anatomy and Physiology Math Chemistry and Medical Microbiology 2nd EditionKaraWalkerixpe100% (39)
- Emergency First Aid and CPRDocument15 pagesEmergency First Aid and CPRvhlactaotaoNo ratings yet
- 3 Bacterial Genetics I & II DentistryDocument90 pages3 Bacterial Genetics I & II DentistryMajd HallakNo ratings yet
- Family Coping IndexDocument5 pagesFamily Coping IndexDarcey NicholeNo ratings yet
- CWTS Final For InstructorDocument147 pagesCWTS Final For Instructorbarbie janeNo ratings yet
- Adrenergic Agonists Classification and EffectsDocument15 pagesAdrenergic Agonists Classification and EffectsSeema YadavNo ratings yet
- Guide To Agriculture Production in Malawi 2021Document448 pagesGuide To Agriculture Production in Malawi 2021william nkhunga100% (3)
- Killer Inside: Aaron Hernandez's Brain DamageDocument3 pagesKiller Inside: Aaron Hernandez's Brain DamageshevarkNo ratings yet
- Beta - Lactam Antibiotics: Prof. R. K. Dixit Pharmacology and Therapeutics K. G. M. U. LucknowDocument29 pagesBeta - Lactam Antibiotics: Prof. R. K. Dixit Pharmacology and Therapeutics K. G. M. U. LucknowHely PatelNo ratings yet
- Dermatology Atlas For Skin ColorDocument300 pagesDermatology Atlas For Skin ColorKiTty Kriss75% (8)
- Pain47, 295Document4 pagesPain47, 295Ezel RitmoNo ratings yet
- June 2022 QP - Component 3 Eduqas Biology A-LevelDocument44 pagesJune 2022 QP - Component 3 Eduqas Biology A-LeveltariffgillNo ratings yet
- 25 OET Official Case Notes (Medicine)Document49 pages25 OET Official Case Notes (Medicine)Mesut KirazNo ratings yet
- Minimally Invasive Shoulder and Elbow Surgery - W. Levine, Et Al., (Informa, 2007) WWDocument408 pagesMinimally Invasive Shoulder and Elbow Surgery - W. Levine, Et Al., (Informa, 2007) WWGeo SanchezNo ratings yet
- Topics: Nasopharyngeal CarcinomaDocument21 pagesTopics: Nasopharyngeal CarcinomaShruthi Y nursingNo ratings yet
- Home Safety For People With Alzheimer's DiseaseDocument44 pagesHome Safety For People With Alzheimer's DiseaseInternational Business Times100% (3)
- Sustainable Livelihoods For Smallholders Farmers in Andhra Pradesh and Uttar PradeshDocument39 pagesSustainable Livelihoods For Smallholders Farmers in Andhra Pradesh and Uttar Pradeshchandra DiveshNo ratings yet
- ComingClean InternetVersionSec.Document168 pagesComingClean InternetVersionSec.Lou DregelyNo ratings yet
- Antisense Oligonucleotide Biotechnology, Applications and FutureDocument29 pagesAntisense Oligonucleotide Biotechnology, Applications and FuturesurojitarpitaNo ratings yet
- Potassium Sulphate vs Potassium Chloride: Their Influence on Crop Yield and QualityDocument109 pagesPotassium Sulphate vs Potassium Chloride: Their Influence on Crop Yield and QualityManuel SosaNo ratings yet
- Pathophysiology For The Health Professions 4th Edition Gould Test BankDocument4 pagesPathophysiology For The Health Professions 4th Edition Gould Test Bankselinadu4in1100% (34)