You might also like
- Cardiovascular Nursing Practice A Comprehensive Resource Manual and Study Guide For Clinical NursesDocument3 pagesCardiovascular Nursing Practice A Comprehensive Resource Manual and Study Guide For Clinical Nursesydtrgn0% (1)
- AP WindowDocument13 pagesAP WindowHugo GonzálezNo ratings yet
- Infective Endocarditis: A Multidisciplinary ApproachFrom EverandInfective Endocarditis: A Multidisciplinary ApproachArman KilicNo ratings yet
- Pamet and PasmethDocument4 pagesPamet and PasmethBash De Guzman50% (2)
- Pacemakers & AICDDocument32 pagesPacemakers & AICDqmmmNo ratings yet
- Nurses Practice in LeukemiaDocument8 pagesNurses Practice in LeukemiaConstantinNo ratings yet
- Assessment and Initial Management Trauma PatientDocument69 pagesAssessment and Initial Management Trauma PatientdrpagrawNo ratings yet
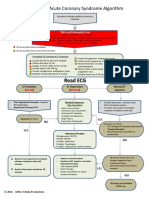
- ACS Algorithm 2016 PDFDocument1 pageACS Algorithm 2016 PDFrabin1994No ratings yet
- ACS - Clinical Review 2015Document11 pagesACS - Clinical Review 2015Purwoko SugengNo ratings yet
- StemiDocument11 pagesStemidoubleraNo ratings yet
- Guide To Clerking 2014Document24 pagesGuide To Clerking 2014Ridhwan Amid100% (1)
- Discuss The Signs and Symptoms Associated With Myocardial InfarctionDocument2 pagesDiscuss The Signs and Symptoms Associated With Myocardial InfarctionDebra YoungbloodNo ratings yet
- Left Ventricular Non-CompactionDocument20 pagesLeft Ventricular Non-CompactionlawlietNo ratings yet
- Patofisiologi AritmiaDocument27 pagesPatofisiologi AritmiaVedora Angelia GultomNo ratings yet
- Chest X Rays Made EasyDocument3 pagesChest X Rays Made EasyHaluk AlibazogluNo ratings yet
- 20 - Toronto Notes 2011 - Ophthamology PDFDocument46 pages20 - Toronto Notes 2011 - Ophthamology PDFSisterzzShopDua0% (1)
- Patho Tree COPDDocument1 pagePatho Tree COPDLaura MitchellNo ratings yet
- Meningitis TBDocument6 pagesMeningitis TBGarrett SimpsonNo ratings yet
- Cad ....Document94 pagesCad ....AnanthibalaNo ratings yet
- Anak 3.1 Infective Endocarditis DRTLTDocument21 pagesAnak 3.1 Infective Endocarditis DRTLTAnastasia PinkyNo ratings yet
- Acute Limb IschaemiaDocument32 pagesAcute Limb IschaemiaAnonymous 9wHscM100% (1)
- Rheumatoid Arthritis Associated Scleritis OPHTHALMOLOGY MCQSDocument5 pagesRheumatoid Arthritis Associated Scleritis OPHTHALMOLOGY MCQSkishorechandraNo ratings yet
- CXR Made EasyDocument14 pagesCXR Made Easyjaimejm100% (1)
- Lutembacher's Syndrome at KolonodaleDocument7 pagesLutembacher's Syndrome at KolonodaleWayan GunawanNo ratings yet
- Gold HallmarkDocument87 pagesGold HallmarkSSGFL1No ratings yet
- Sickle Cell Disease: Everything You Ever Wanted To KnowDocument23 pagesSickle Cell Disease: Everything You Ever Wanted To KnowAnastasiafynn100% (1)
- ENT Quick ReviewDocument6 pagesENT Quick ReviewWade100% (1)
- Short Case 1 PterygiumDocument15 pagesShort Case 1 PterygiumAnmol KhadkaNo ratings yet
- EcmoDocument81 pagesEcmoBasantkumar SinghNo ratings yet
- Special Sense System Group 6Document24 pagesSpecial Sense System Group 6RushdaNo ratings yet
- Daftar Kode Diagnosa & TindakanDocument7 pagesDaftar Kode Diagnosa & Tindakannovi andriyaniNo ratings yet
- Cardiovascular Nursing: Study Online atDocument7 pagesCardiovascular Nursing: Study Online atLilly DayeNo ratings yet
- Sickle Cell Disease: Click To Edit Master Subtitle StyleDocument13 pagesSickle Cell Disease: Click To Edit Master Subtitle StyleAditya Rangga Fandiarta100% (1)
- Pericardial EffusionDocument3 pagesPericardial EffusionNita Hurek100% (1)
- Icd XDocument3 pagesIcd XR Ghianesya GantinaNo ratings yet
- Acid-Base Disorders NotesDocument10 pagesAcid-Base Disorders NotesLovely100% (1)
- Management of Cardiac Disease in PregnancyDocument12 pagesManagement of Cardiac Disease in Pregnancyapi-3705046No ratings yet
- Arterial LinesDocument9 pagesArterial LinesRei IrincoNo ratings yet
- Acute Coronary SyndromeDocument23 pagesAcute Coronary SyndromeThanujaa UvarajNo ratings yet
- Spectrum of Acute Coronary Syndrome: Milagros Estrada-Yamamoto, MDDocument62 pagesSpectrum of Acute Coronary Syndrome: Milagros Estrada-Yamamoto, MDAnonymous HH3c17osNo ratings yet
- Ventikular Septal Defect FixDocument18 pagesVentikular Septal Defect FixPutri Sari DewiNo ratings yet
- Central Line PlacementDocument49 pagesCentral Line PlacementAndresPimentelAlvarezNo ratings yet
- Cardio-Vascular Disease: Mitral Stenosis & Mitral RegurgitationDocument25 pagesCardio-Vascular Disease: Mitral Stenosis & Mitral Regurgitationyulia silviNo ratings yet
- Pedi Pearls 2 - Scrubed PDFDocument46 pagesPedi Pearls 2 - Scrubed PDFthomasfx10100% (1)
- Aortic StenosisDocument3 pagesAortic StenosisMaxine BaraquiaNo ratings yet
- Sgarbossa CriteriaDocument5 pagesSgarbossa Criteriajacknaim7090No ratings yet
- Pulmonary Diseases - Dental ManagementDocument45 pagesPulmonary Diseases - Dental Managementfilyouth4life100% (3)
- Atrial ExtrasystoleDocument11 pagesAtrial ExtrasystoleRaiganNo ratings yet
- Monitoring Intra Operatif: Mindi Widayani NRP 122.022.1115 FK UPN "Veteran" JakartaDocument21 pagesMonitoring Intra Operatif: Mindi Widayani NRP 122.022.1115 FK UPN "Veteran" Jakartaputri wulandariNo ratings yet
- Case Report STEMI Inferior PosteriorDocument38 pagesCase Report STEMI Inferior PosteriorNorazeela BaharudinNo ratings yet
- Aortic Stenosis Differential DiagnosisDocument12 pagesAortic Stenosis Differential DiagnosisCristina PorfireNo ratings yet
- EKG InterpretationDocument63 pagesEKG InterpretationMiriam Cindy MathullaNo ratings yet
- Anamnesis & PemfisDocument81 pagesAnamnesis & PemfisFikriYTNo ratings yet
- 7.1 Gradual Loss of VisionDocument19 pages7.1 Gradual Loss of VisionparugandooNo ratings yet
- Cardiac Emergency PDFDocument45 pagesCardiac Emergency PDFnikenNo ratings yet
- Skin and Soft Tissue Infectons 1Document51 pagesSkin and Soft Tissue Infectons 1AISHWARYA T DNo ratings yet
- Anatomi JantungDocument2 pagesAnatomi JantungAuliya NaimahNo ratings yet
- Valvular Heart Disease: Aortic StenosisDocument28 pagesValvular Heart Disease: Aortic StenosisRajiv_Saikia_3577100% (1)
- Unit Two The Health Benefits of Physical ActivityDocument10 pagesUnit Two The Health Benefits of Physical ActivityYoseph DefaruNo ratings yet
- Defects Lamellar TearingDocument6 pagesDefects Lamellar Tearingguru_terexNo ratings yet
- Pure Vegeterian: Kousika (CaterersDocument2 pagesPure Vegeterian: Kousika (CaterersShylender NagaNo ratings yet
- DDEV SPICES PVT LTD (Product List)Document1 pageDDEV SPICES PVT LTD (Product List)jaymin zalaNo ratings yet
- Low Voltage Fixed and Automatic Power Factor Correction SystemsDocument6 pagesLow Voltage Fixed and Automatic Power Factor Correction Systemszabiruddin786No ratings yet
- Ethics, Privacy, and Security: Lesson 14Document16 pagesEthics, Privacy, and Security: Lesson 14Jennifer Ledesma-Pido100% (1)
- Learning Activity Sheet MAPEH 10 (P.E.) : First Quarter/Week 1Document4 pagesLearning Activity Sheet MAPEH 10 (P.E.) : First Quarter/Week 1Catherine DubalNo ratings yet
- Containers HandbookDocument26 pagesContainers Handbookrishi vohraNo ratings yet
- Sampoong Department Store - A Literary Critique (Mimetic Theory)Document2 pagesSampoong Department Store - A Literary Critique (Mimetic Theory)Ron Marc CaneteNo ratings yet
- Lab CompilationDocument11 pagesLab CompilationJanita SiddiquiNo ratings yet
- Evidence-Based Strength & HypertrophyDocument6 pagesEvidence-Based Strength & HypertrophyAnže BenkoNo ratings yet
- Risk Appetite PresentationDocument10 pagesRisk Appetite PresentationAntonyNo ratings yet
- EBANX Beyond Borders 2020Document71 pagesEBANX Beyond Borders 2020Fernanda MelloNo ratings yet
- Fawad Hussain, Feedback On Industrial Visit To Sahiwal Coal Power PlantDocument2 pagesFawad Hussain, Feedback On Industrial Visit To Sahiwal Coal Power PlantSyed Fawad MarwatNo ratings yet
- Industrial Visit ReportDocument8 pagesIndustrial Visit ReportAnuragBoraNo ratings yet
- Sociology/Marriage PresentationDocument31 pagesSociology/Marriage PresentationDoofSadNo ratings yet
- Hotel Elizabeth in Baguio City: Address: J Felipe Street Cor. Gibraltar Road Mines View Park, Baguio City, PhilippinesDocument16 pagesHotel Elizabeth in Baguio City: Address: J Felipe Street Cor. Gibraltar Road Mines View Park, Baguio City, PhilippinesI amEllaNo ratings yet
- Margarita ForesDocument20 pagesMargarita ForesKlarisse YoungNo ratings yet
- Transformers: Z Z Z S S Z S SDocument17 pagesTransformers: Z Z Z S S Z S SSreenivasaraoDharmavarapu100% (1)
- Vocab PDFDocument29 pagesVocab PDFShahab SaqibNo ratings yet
- Top 6 Beginner Work Out MistakesDocument4 pagesTop 6 Beginner Work Out MistakesMARYAM GULNo ratings yet
- Chef Basics Favorite RecipesDocument58 pagesChef Basics Favorite Recipesbillymac303a100% (2)
- 7 LevelDocument5 pages7 LevelACHREF RIHANINo ratings yet
- Transmission Lines SMART EDGE VILLARUEL For April 2024 v1Document89 pagesTransmission Lines SMART EDGE VILLARUEL For April 2024 v1mayandichoso24No ratings yet
- Rrs PresentationDocument69 pagesRrs PresentationPriyamvada Biju100% (1)
- Ergo 1 - Workshop 3Document3 pagesErgo 1 - Workshop 3Mugar GeillaNo ratings yet
- Main CatalogueDocument12 pagesMain Catalogueferpa_ferNo ratings yet
- Plasma Arc Machining (Pam) : Mechanical Engineering Department I.I.T Guwahati-781039 E-Mail: Manasdas@iitg - Ernet.inDocument15 pagesPlasma Arc Machining (Pam) : Mechanical Engineering Department I.I.T Guwahati-781039 E-Mail: Manasdas@iitg - Ernet.inSrinivasanNo ratings yet
- Environmental Research and Public Health: International Journal ofDocument12 pagesEnvironmental Research and Public Health: International Journal ofKarenNo ratings yet