You might also like
- Air Ticket Booking - Book Flight Tickets - Cheap Air Fare - LTC Fare - IRCTC AIRDocument2 pagesAir Ticket Booking - Book Flight Tickets - Cheap Air Fare - LTC Fare - IRCTC AIRMohitSharmaNo ratings yet
- Vijaya Diagnostic Lab Test ReportDocument1 pageVijaya Diagnostic Lab Test ReportUpender Rao SunkishalaNo ratings yet
- Attendance Challenge ToolkitDocument19 pagesAttendance Challenge Toolkitapi-197489652No ratings yet
- Ann Soehee - Tctap2021 - SPCDocument43 pagesAnn Soehee - Tctap2021 - SPCSaad KhanNo ratings yet
- Management of Dyslipidemia and The Prevention of Cardiovascular DiseaseDocument2 pagesManagement of Dyslipidemia and The Prevention of Cardiovascular DiseaseBenny TrisaktyariNo ratings yet
- Dyslipidaemia 2019Document61 pagesDyslipidaemia 2019fatima.shqeratNo ratings yet
- Lower Is Better - FinalDocument91 pagesLower Is Better - FinalJamsidul Hassan RajibNo ratings yet
- Asap LipidDocument131 pagesAsap LipidagassiNo ratings yet
- Management of Blood Cholesterol 2019Document2 pagesManagement of Blood Cholesterol 2019Luis Alberto Alvarez AnkassNo ratings yet
- 2019 - ESC - Guidelines SLIDESDocument23 pages2019 - ESC - Guidelines SLIDESFa CurieNo ratings yet
- What's New in Lipid GuidelinesDocument31 pagesWhat's New in Lipid GuidelinesYunita WidyaningsihNo ratings yet
- HYPERLIPIDEMIADocument33 pagesHYPERLIPIDEMIAatiqullah tarmiziNo ratings yet
- Triglycerides and VLDL: (Increased Ra Tio of Triglyceride To Apob)Document20 pagesTriglycerides and VLDL: (Increased Ra Tio of Triglyceride To Apob)Indah Pujiati DtNo ratings yet
- Dyslipidemias: Abdullah Al-Dahbali, Mpharm, PHDDocument15 pagesDyslipidemias: Abdullah Al-Dahbali, Mpharm, PHDعزالدين الطيارNo ratings yet
- RX For Selected PtsDocument22 pagesRX For Selected PtsBubu ToNo ratings yet
- Nicotinic Acid 10-20% 10-20% 14-35% 30-70% Reasonable To PoorDocument5 pagesNicotinic Acid 10-20% 10-20% 14-35% 30-70% Reasonable To PoorvmvlivNo ratings yet
- Guidelines DyslipidDocument49 pagesGuidelines Dyslipidnoveldycb89No ratings yet
- ADA and AACE Guideline Updates: 10 Key ChangesDocument27 pagesADA and AACE Guideline Updates: 10 Key ChangesKarthik SNo ratings yet
- Lower is Better: No Evidence for Treating to Specific lipid TargetsDocument91 pagesLower is Better: No Evidence for Treating to Specific lipid TargetsJamsidul Hassan RajibNo ratings yet
- Lower Is Better - No Evidence For Treating To Spepecific Lipid Targets & Use of StatinsDocument59 pagesLower Is Better - No Evidence For Treating To Spepecific Lipid Targets & Use of StatinsJamsidul Hassan RajibNo ratings yet
- Clinical Pharmacy Department Clinical Pharmacy and Drug Information PL 504Document61 pagesClinical Pharmacy Department Clinical Pharmacy and Drug Information PL 504Bassant Ahmed Mahmoud Ragab Abdallah AyaadNo ratings yet
- HyperlipidemiaDocument38 pagesHyperlipidemiaAadhan ArveeNo ratings yet
- Hi Per Colesterol Emi ADocument38 pagesHi Per Colesterol Emi AFernando ArancibiaNo ratings yet
- Pediatric Patients (10-17 Years of Age)Document18 pagesPediatric Patients (10-17 Years of Age)asdwasdNo ratings yet
- Patient-Centered Statins Guideline Simplifies ASCVD Risk AssessmentDocument51 pagesPatient-Centered Statins Guideline Simplifies ASCVD Risk Assessmentdr_yasserNo ratings yet
- Dyslipidemia ATP4 GUIDLINESDocument9 pagesDyslipidemia ATP4 GUIDLINESSandy GunawanNo ratings yet
- Treatment of Lipid Disorders-SchubartDocument76 pagesTreatment of Lipid Disorders-SchubartOliver OwuorNo ratings yet
- Roseday EZ Webinar SlidesDocument35 pagesRoseday EZ Webinar SlidesPragnesh ShahNo ratings yet
- Dyslipidemia: Dr. Sohail AhmadDocument36 pagesDyslipidemia: Dr. Sohail AhmadChong Zhi LinNo ratings yet
- Dr. Endah Dewati K.S. SPJPDocument41 pagesDr. Endah Dewati K.S. SPJPbudiantoNo ratings yet
- 2018 Clinical Practice Guidelines: Diabetes in Older PeopleDocument35 pages2018 Clinical Practice Guidelines: Diabetes in Older Peopledodi ikhsanNo ratings yet
- Niacin: or Nicotinic AcidDocument20 pagesNiacin: or Nicotinic AcidPandiya RajaNo ratings yet
- Guidelines for managing hypertension and diabetesDocument8 pagesGuidelines for managing hypertension and diabeteschandra9000No ratings yet
- 4.investigations of Serum LipidsDocument7 pages4.investigations of Serum LipidsMV ProductionNo ratings yet
- UgpeDocument3 pagesUgpeOlety Subrahmanya SastryNo ratings yet
- 2013 Cholesterol Guidelines at A Glance: - Robert Barnes, M3Document15 pages2013 Cholesterol Guidelines at A Glance: - Robert Barnes, M3CoolrobertizNo ratings yet
- The Control of The Glucose Triad - ChallengesDocument26 pagesThe Control of The Glucose Triad - ChallengesDigei BobitzNo ratings yet
- A Comprehensive Review On Metabolic SyndromeDocument41 pagesA Comprehensive Review On Metabolic Syndromeveerraju tvNo ratings yet
- Dislipidemia: Ulvi Nur RistaDocument29 pagesDislipidemia: Ulvi Nur RistaYogie 1290No ratings yet
- Recommendations For The Intensity of Statin Therapy Based On Statin Benefit Group Diagram. (AdaptedDocument8 pagesRecommendations For The Intensity of Statin Therapy Based On Statin Benefit Group Diagram. (Adaptedعزالدين الطيارNo ratings yet
- 8 - Lipoprotéines 3Document21 pages8 - Lipoprotéines 3nour achkarNo ratings yet
- New Developments in The Management of Dyslipidemia: Widjanarko. W MDDocument62 pagesNew Developments in The Management of Dyslipidemia: Widjanarko. W MDyulanda fitrianaNo ratings yet
- Understanding The Needs of The High Productive DyslipidemiaDocument47 pagesUnderstanding The Needs of The High Productive DyslipidemiachchchchkNo ratings yet
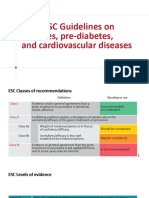
- 2019 ESC Guidelines On Diabetes, Pre-Diabetes, and Cardiovascular DiseasesDocument19 pages2019 ESC Guidelines On Diabetes, Pre-Diabetes, and Cardiovascular DiseasesBertha MansurNo ratings yet
- Lipids Topic DiscussionDocument10 pagesLipids Topic Discussionapi-665372449No ratings yet
- Medical Check Up Standard Operating Procedure For Diagnosis 1. BMIDocument25 pagesMedical Check Up Standard Operating Procedure For Diagnosis 1. BMIlita agustinNo ratings yet
- MG/DL MG/DL MG/DL MG/DL MG/DL MG/DLDocument3 pagesMG/DL MG/DL MG/DL MG/DL MG/DL MG/DLAli Shaikh AbdulNo ratings yet
- NCEP Hyperlipidemia GoalsDocument6 pagesNCEP Hyperlipidemia GoalsVictoria Eliza InguilloNo ratings yet
- Evolution of Lipid Management GuidelinesDocument63 pagesEvolution of Lipid Management GuidelinesM Azmi HNo ratings yet
- Cholesterol Guidelines Review 2020Document6 pagesCholesterol Guidelines Review 2020oriannaocantoNo ratings yet
- New Recommendations and Revised Concepts in Recent Guidelines On The Management of Dyslipidemias To Prevent Cardiovascular Disease-The 2018 ACC-AHA and 2019 ESC-EAS GuidelinesDocument6 pagesNew Recommendations and Revised Concepts in Recent Guidelines On The Management of Dyslipidemias To Prevent Cardiovascular Disease-The 2018 ACC-AHA and 2019 ESC-EAS GuidelinesJustinaNo ratings yet
- Biochemistry Practical RGKSUDocument43 pagesBiochemistry Practical RGKSUmuhammad umer abdul moizNo ratings yet
- Hyperlipidemia: Brian V. Reamy, MD, Colonel, USAF, MC Chair - Department of Family Medicine Uniformed Services UniversityDocument58 pagesHyperlipidemia: Brian V. Reamy, MD, Colonel, USAF, MC Chair - Department of Family Medicine Uniformed Services Universityayloleh87No ratings yet
- Dyslipidemia - 2Document17 pagesDyslipidemia - 2Mohamed AbouzaidNo ratings yet
- DyslipidemiaDocument21 pagesDyslipidemiaBasil HussamNo ratings yet
- Vijaya Diagnostic Centre Lipid Profile Test ReportDocument1 pageVijaya Diagnostic Centre Lipid Profile Test Reportnagakiran9No ratings yet
- DR - Dr. Seobagijo Adi, SpPD-KEMD-Segi Prakteis Panduan Pemilihan Obat Oral Anti DiabetesDocument31 pagesDR - Dr. Seobagijo Adi, SpPD-KEMD-Segi Prakteis Panduan Pemilihan Obat Oral Anti DiabetesraraNo ratings yet
- Laboratory Test Report: Male 16 YearsDocument3 pagesLaboratory Test Report: Male 16 YearsChandrika VeerareddyNo ratings yet
- Experiment On Lipid Profile: Sec 1C Group 4Document18 pagesExperiment On Lipid Profile: Sec 1C Group 4ned_fanerNo ratings yet
- Nutrition of The Cardiovasculer System: Syarif Husin Blok 10Document37 pagesNutrition of The Cardiovasculer System: Syarif Husin Blok 10Desi OktarianaNo ratings yet
- K20. DNA Forensik - Dr. Virhan, M.BiomedDocument20 pagesK20. DNA Forensik - Dr. Virhan, M.BiomedLia pramitaNo ratings yet
- Critical Appraisal Cross-Sectional SurveyDocument1 pageCritical Appraisal Cross-Sectional SurveyNur Vicka VickaNo ratings yet
- Time Table-1-1Document3 pagesTime Table-1-1Lia pramitaNo ratings yet
- Jadwal 1 Februari FixDocument4 pagesJadwal 1 Februari FixLia pramitaNo ratings yet
- K28. Malpraktek - Dr. Monang, SP.FDocument18 pagesK28. Malpraktek - Dr. Monang, SP.FLia pramitaNo ratings yet
- ESC Guidelines For DX and TX of Acute and Chronic HF (2016)Document85 pagesESC Guidelines For DX and TX of Acute and Chronic HF (2016)Imja94No ratings yet
- Steno Ciii StenoDocument21 pagesSteno Ciii StenoLia pramitaNo ratings yet
- Prevention Guidelines Made SimpleDocument17 pagesPrevention Guidelines Made SimplearseniosilvaNo ratings yet
- K3. Penatalaksanaan Kasus Neurologi Di FKTP - Dr. Achmad Faqih, SP.SDocument30 pagesK3. Penatalaksanaan Kasus Neurologi Di FKTP - Dr. Achmad Faqih, SP.SLia pramitaNo ratings yet
- Ehz 467Document65 pagesEhz 467Coy Calapatia-TorresNo ratings yet
- Gout and Othercrystal-Associated ArthropathiesDocument31 pagesGout and Othercrystal-Associated ArthropathiesLia pramitaNo ratings yet
- 388tetanus For Website PDFDocument52 pages388tetanus For Website PDFLia pramitaNo ratings yet
- Myeloid LeukemiaDocument36 pagesMyeloid LeukemiaLia pramitaNo ratings yet
- Lung Abscess: DR Budi Enoch SPPDDocument14 pagesLung Abscess: DR Budi Enoch SPPDLia pramitaNo ratings yet
- Lymphoid Lekemia: DR Budi Enoch SPPDDocument32 pagesLymphoid Lekemia: DR Budi Enoch SPPDLia pramitaNo ratings yet
- Systemic Lupus Erythematosus (SLE)Document62 pagesSystemic Lupus Erythematosus (SLE)Lia pramitaNo ratings yet
- Periarticular Disorders of The ExtremitiesDocument20 pagesPeriarticular Disorders of The ExtremitiesLia pramitaNo ratings yet
- Atherosklerosis: DR Budi Enoch SPPDDocument56 pagesAtherosklerosis: DR Budi Enoch SPPDLia pramitaNo ratings yet
- Systrmic Lupus Erythematosus (Sle)Document62 pagesSystrmic Lupus Erythematosus (Sle)Dedy Santoso ChouNo ratings yet
- Coagulation DisordersDocument26 pagesCoagulation DisordersLia pramitaNo ratings yet
- Atherosklerosis: DR Budi Enoch SPPDDocument56 pagesAtherosklerosis: DR Budi Enoch SPPDLia pramitaNo ratings yet
- Gout and Othercrystal-Associated ArthropathiesDocument31 pagesGout and Othercrystal-Associated ArthropathiesLia pramitaNo ratings yet
- Coagulation DisordersDocument26 pagesCoagulation DisordersLia pramita0% (1)
- Gout and Othercrystal-Associated ArthropathiesDocument31 pagesGout and Othercrystal-Associated ArthropathiesLia pramitaNo ratings yet
- Geriatric Medicine KuliahDocument38 pagesGeriatric Medicine KuliahLia pramitaNo ratings yet
- 5 Pain Management in The Elderly PopulationDocument26 pages5 Pain Management in The Elderly PopulationLia pramitaNo ratings yet
- Hemoglobinopathy Dan Sindroma ThalasemiaDocument62 pagesHemoglobinopathy Dan Sindroma ThalasemiaLia pramitaNo ratings yet
- Glucose and Dementia - Geriatri JurnalDocument20 pagesGlucose and Dementia - Geriatri JurnalLia pramitaNo ratings yet
- 4 Palliative CareDocument35 pages4 Palliative CareLia pramitaNo ratings yet
- CP306 Example 01 OKDocument5 pagesCP306 Example 01 OKManish MahadevwalaNo ratings yet
- Empowerment Is A Leadership TrickDocument10 pagesEmpowerment Is A Leadership TrickAura Carla TolentinoNo ratings yet
- Surface Modification of Titanium Orthodontic ImplaDocument30 pagesSurface Modification of Titanium Orthodontic ImplaMary SmileNo ratings yet
- Ultra-compact Terrier drilling rig fits through standard doorwaysDocument8 pagesUltra-compact Terrier drilling rig fits through standard doorwaysjpantazis1975No ratings yet
- PTR 326 Theoretical Lecture 1Document14 pagesPTR 326 Theoretical Lecture 1muhammedariwanNo ratings yet
- 1ST Quarter Exam Mapeh 8Document7 pages1ST Quarter Exam Mapeh 8John Rey Manolo BaylosisNo ratings yet
- 6.4 Qualitative Quantitative AnalysisDocument6 pages6.4 Qualitative Quantitative AnalysisAndrea PagsuguironNo ratings yet
- Cost Concepts, Cost Analysis, and Cost EstimationDocument2 pagesCost Concepts, Cost Analysis, and Cost EstimationGêmTürÏngånÖNo ratings yet
- BMEn 3301 Spring 2013 SyllabusDocument13 pagesBMEn 3301 Spring 2013 SyllabussfairhuNo ratings yet
- Does Dataset Complexity Matters For Model Explainers?: 1 Jos e Ribeiro 2 Ra Issa Silva 3 Lucas CardosoDocument9 pagesDoes Dataset Complexity Matters For Model Explainers?: 1 Jos e Ribeiro 2 Ra Issa Silva 3 Lucas CardosoJoão PauloNo ratings yet
- Guided Noteboo Kin GED10 2 (Mathe Matics in The Modern World)Document5 pagesGuided Noteboo Kin GED10 2 (Mathe Matics in The Modern World)Aaronie DeguNo ratings yet
- Bahan Belajar Ujian Akhir SekolahDocument13 pagesBahan Belajar Ujian Akhir SekolahArga AnggaraNo ratings yet
- Ginger by NcipmDocument53 pagesGinger by NcipmAbhishekNo ratings yet
- MCAS Forces and Equilibrium PracticeDocument51 pagesMCAS Forces and Equilibrium PracticeSyd MalaxosNo ratings yet
- Ec6303 Signals and SystemsDocument2 pagesEc6303 Signals and SystemsSam PaulNo ratings yet
- Lab Manual Ds&BdalDocument100 pagesLab Manual Ds&BdalSEA110 Kshitij BhosaleNo ratings yet
- E - Efma Rbi Insp Interval Assess Projector - PP SimtechDocument10 pagesE - Efma Rbi Insp Interval Assess Projector - PP SimtechAbhimanyu SharmaNo ratings yet
- HIST 1010 EXAM 3 TEST PREP (With Answers)Document2 pagesHIST 1010 EXAM 3 TEST PREP (With Answers)Ophelia ThorntonNo ratings yet
- Parts List of Engine Assy Ofdz-00536Document1 pageParts List of Engine Assy Ofdz-00536CwsNo ratings yet
- Process Payments & ReceiptsDocument12 pagesProcess Payments & ReceiptsAnne FrondaNo ratings yet
- Psv5 FHD 215naDocument1 pagePsv5 FHD 215naVijay BhureNo ratings yet
- PP 1Document33 pagesPP 1Vishnu IngleNo ratings yet
- Weak Downlink Data for Multiple TRX Indices Over TimeDocument3,643 pagesWeak Downlink Data for Multiple TRX Indices Over TimeSK Basak BDNo ratings yet
- Case 26 Star River Electronics - Group Thạch Trung Chương HiểnDocument12 pagesCase 26 Star River Electronics - Group Thạch Trung Chương HiểnTrương ThạchNo ratings yet
- Chapter 2. COST IDocument8 pagesChapter 2. COST IyebegashetNo ratings yet
- Making Charts With Excel 2003: Income & ProfitDocument9 pagesMaking Charts With Excel 2003: Income & ProfitArunNo ratings yet
- Studies on the vertically barred Haplochromis electra from Lake MalawiDocument5 pagesStudies on the vertically barred Haplochromis electra from Lake MalawiCenk Sururi KarabulutNo ratings yet
- WME01 01 Que 20220510Document15 pagesWME01 01 Que 20220510muhammad awaisNo ratings yet