You might also like
- NbmeDocument5 pagesNbmeRahul ShuklaNo ratings yet
- Prostate GlandsDocument3 pagesProstate GlandsDragan PetrovicNo ratings yet
- Lecture 124 MALE INFERTILITY by Dr. NayyerDocument63 pagesLecture 124 MALE INFERTILITY by Dr. NayyerRizwan AhmedNo ratings yet
- OSCE Gynae HXDocument3 pagesOSCE Gynae HXmpage3100% (1)
- Ovaries and Ovarian TumoursDocument121 pagesOvaries and Ovarian TumoursMujeeb MNo ratings yet
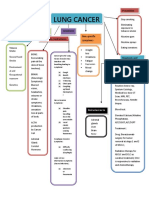
- Concept Map LungDocument1 pageConcept Map LungThea Eya FayeNo ratings yet
- MCQs Ch07-45651100rdzDocument27 pagesMCQs Ch07-45651100rdzKhalifa AL-Wishahi100% (2)
- Salvestrols Cures CancerDocument29 pagesSalvestrols Cures CancerJohn Tan100% (1)
- Oncology NursingDocument10 pagesOncology NursingJean AustenNo ratings yet
- Penile Cancer 2010Document28 pagesPenile Cancer 2010raghavagummadiNo ratings yet
- SMRT Radiation Therapy IntroDocument18 pagesSMRT Radiation Therapy IntroDar WebNo ratings yet
- Tumor Urogenital: Dr. Alvarino SPB SpuDocument41 pagesTumor Urogenital: Dr. Alvarino SPB SpuDita Azzahra SupraptoNo ratings yet
- Tumor Urogenital: Dr. Hariyono, SpuDocument42 pagesTumor Urogenital: Dr. Hariyono, SpumelianyNo ratings yet
- Lecture 26. RCC, Adrenal, Wiims TumorDocument31 pagesLecture 26. RCC, Adrenal, Wiims TumorkrisnadewirahadiNo ratings yet
- DR 180114164748Document43 pagesDR 180114164748Hasnain ToheedNo ratings yet
- Ferrets Oncology-MainDocument26 pagesFerrets Oncology-MainJOAQUINALONZOPEREIRANo ratings yet
- Testicular Tumours Part1Document16 pagesTesticular Tumours Part1luckyswiss7776848No ratings yet
- Block 3.3 Sesi 3 Pathology of Urinary Tract: by Asdos 2011: Vetta Awe Eric Lily Fiko Ghana Ikal Linda May FahmiDocument96 pagesBlock 3.3 Sesi 3 Pathology of Urinary Tract: by Asdos 2011: Vetta Awe Eric Lily Fiko Ghana Ikal Linda May Fahmimail junkNo ratings yet
- Renal Cell CarcinomaDocument56 pagesRenal Cell CarcinomaBONG AIKCHINGNo ratings yet
- Thediagnosisand Managementof Scrotalmasses: Jeffrey S. Montgomery,, David A. BloomDocument10 pagesThediagnosisand Managementof Scrotalmasses: Jeffrey S. Montgomery,, David A. BloomLyka MahrNo ratings yet
- Tumor IntraabdomenDocument30 pagesTumor IntraabdomenBedahanakugmNo ratings yet
- Female GUDocument18 pagesFemale GULauren LaMonicaNo ratings yet
- Kartagner Syndrom ICSI OutcomDocument16 pagesKartagner Syndrom ICSI OutcomWael BadranNo ratings yet
- AMENORRHOEADocument16 pagesAMENORRHOEAdrravindermehetreyNo ratings yet
- Gynecologic Cancers: Cervix, Uterus, and OvaryDocument43 pagesGynecologic Cancers: Cervix, Uterus, and Ovaryraul sinatoNo ratings yet
- Tumor Urogenital NandaDocument41 pagesTumor Urogenital NandaKerisnandaMcPissleyNo ratings yet
- Varicocele: Causes and Surgical TreatmentDocument56 pagesVaricocele: Causes and Surgical TreatmentMuhammad MakkiNo ratings yet
- Testicular Cancer Screening and DiagnosisDocument44 pagesTesticular Cancer Screening and DiagnosisYazeed AsrawiNo ratings yet
- Overview Diagnosis and Treatment of GI NETSDocument73 pagesOverview Diagnosis and Treatment of GI NETSΒΑΣΙΛΗΣ ΚΟΛΙΝΤΖΙΚΗΣNo ratings yet
- NEOPLASIADocument15 pagesNEOPLASIADr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Principles of Neoplasia (New)Document125 pagesPrinciples of Neoplasia (New)egyfellowpathologyNo ratings yet
- Dr. Dr. Tjokorda Gde, SP - PD KEMD-Thyroid NoduleDocument51 pagesDr. Dr. Tjokorda Gde, SP - PD KEMD-Thyroid NodulevinahandoyoNo ratings yet
- Cancer: By: Carolina Vidal, RNDocument49 pagesCancer: By: Carolina Vidal, RNCarolina VidalNo ratings yet
- Cancer Nursing: By: Mrs. Theresa Margarita Marivee L. SaldevarDocument24 pagesCancer Nursing: By: Mrs. Theresa Margarita Marivee L. Saldevarfaithfabulous1_06100% (2)
- Accepted Manuscript: UrologyDocument12 pagesAccepted Manuscript: UrologyayunikmatulNo ratings yet
- Multiple Endocrine NeoplasiaDocument4 pagesMultiple Endocrine NeoplasiaDivya RanasariaNo ratings yet
- Testicles Research by Deez Part 1Document23 pagesTesticles Research by Deez Part 1Dark flame masterNo ratings yet
- Patologi Tumor Sistim UrogenitalDocument29 pagesPatologi Tumor Sistim UrogenitalSiddiq Blackhell CakepNo ratings yet
- NEOPLASMA (1Document65 pagesNEOPLASMA (1Syeila marselaNo ratings yet
- Importatn Topics REPRO M13Document9 pagesImportatn Topics REPRO M13idzniNo ratings yet
- Student'S Gynaecology Notes: For Students, by StudentsDocument45 pagesStudent'S Gynaecology Notes: For Students, by StudentsAdli IsmailNo ratings yet
- Assessment and Diagnosis of Abdominal Masses in Children: Resident Education Lecture SeriesDocument45 pagesAssessment and Diagnosis of Abdominal Masses in Children: Resident Education Lecture SeriesboubiyouNo ratings yet
- UrinaraDocument71 pagesUrinaraBad AssNo ratings yet
- A2 Prostate Ca - AinDocument4 pagesA2 Prostate Ca - AinNur Liyana Ahmad ZakiNo ratings yet
- A Curious Case of Persistent Mullerian Duct Syndrome (PMDS) With Seminoma: A Report of A Rare CaseDocument6 pagesA Curious Case of Persistent Mullerian Duct Syndrome (PMDS) With Seminoma: A Report of A Rare Casecommon 9943No ratings yet
- Tumor Pada Ginjal: Dr.H.Delyuzar, M.Ked (Pa), Sppa (K)Document134 pagesTumor Pada Ginjal: Dr.H.Delyuzar, M.Ked (Pa), Sppa (K)Dony DamaraNo ratings yet
- Carcinosarcoma of The Parotid Gland: Case ReportDocument42 pagesCarcinosarcoma of The Parotid Gland: Case ReportrohinmNo ratings yet
- PA - Dasar Neoplasma (DrBerti) PDFDocument67 pagesPA - Dasar Neoplasma (DrBerti) PDFElearning FK UnhasNo ratings yet
- Oncology StarsDocument61 pagesOncology StarsCharles Conrad Pagcaliwagan BagsitNo ratings yet
- DR Mohamed Saber DR Jeremy Jones: Testicular MicrolithiasisDocument5 pagesDR Mohamed Saber DR Jeremy Jones: Testicular MicrolithiasisJean NgNo ratings yet
- Morpho Lectures Merged Reproductive System PDFDocument204 pagesMorpho Lectures Merged Reproductive System PDFapNo ratings yet
- Infertility: by Kenbon SDocument58 pagesInfertility: by Kenbon SgimNo ratings yet
- Onco - Day 1 Final SVDocument170 pagesOnco - Day 1 Final SVApril Mae Magos LabradorNo ratings yet
- BPH PSPD 2012Document43 pagesBPH PSPD 2012Nor AinaNo ratings yet
- (#3) Primary and Secondary Sex Differentiation-2016Document54 pages(#3) Primary and Secondary Sex Differentiation-2016marina_shawkyNo ratings yet
- Approach To Endometrial BiopsyDocument62 pagesApproach To Endometrial BiopsySumiya JssalbNo ratings yet
- Urogenital Embryology & AnatomyDocument93 pagesUrogenital Embryology & Anatomydr.hendraNo ratings yet
- 4 - ProstateDocument9 pages4 - ProstateHardiTariqHammaNo ratings yet
- Genpath NeoplasiaDocument35 pagesGenpath Neoplasiajulo_05No ratings yet
- 3.1.5.3 Patologi Anatomi Sistem Urogenital Dan PayudaraDocument70 pages3.1.5.3 Patologi Anatomi Sistem Urogenital Dan PayudaraaiysahmirzaNo ratings yet
- Female Reproductive - 3, Dub, Uterus Lesions, Turner SyndromeDocument34 pagesFemale Reproductive - 3, Dub, Uterus Lesions, Turner Syndromeindu mathiNo ratings yet
- Presentation Ectopic HormonesDocument12 pagesPresentation Ectopic HormonesCritic CrazzyNo ratings yet
- Neuroendocrine Tumors: Surgical Evaluation and ManagementFrom EverandNeuroendocrine Tumors: Surgical Evaluation and ManagementJordan M. CloydNo ratings yet
- ESM e Ne BreastDocument60 pagesESM e Ne BreastNiv SabathNo ratings yet
- Cancer Cells: How They Start and CharacteristicsDocument7 pagesCancer Cells: How They Start and CharacteristicsARISNo ratings yet
- Scribd Is The WorstDocument1 pageScribd Is The WorstFuck YouNo ratings yet
- Cervical Cancer Screening - DOH Standard - May 2018Document14 pagesCervical Cancer Screening - DOH Standard - May 2018Basil al-hashaikehNo ratings yet
- Ovarian Tumours: Epidemiology, Risk Factors, Classification, and ManagementDocument49 pagesOvarian Tumours: Epidemiology, Risk Factors, Classification, and ManagementChoden JamyangNo ratings yet
- Cervical Cancer Awareness MonthDocument16 pagesCervical Cancer Awareness MonthParpar IparNo ratings yet
- Presentation and Management of Intracranial Space Occupying Lesions (Icsol)Document66 pagesPresentation and Management of Intracranial Space Occupying Lesions (Icsol)heruNo ratings yet
- Mouth Cancer Information LeafletDocument2 pagesMouth Cancer Information LeafletmukeshrinkNo ratings yet
- Laryngeal Tumor Types and TreatmentsDocument72 pagesLaryngeal Tumor Types and TreatmentsYuliana SariNo ratings yet
- CP Breast Invasive Biopsy 19 1001Document9 pagesCP Breast Invasive Biopsy 19 1001Rajeev PareekNo ratings yet
- MR Imaging of Tumor and Tumorlike Lesions ofDocument43 pagesMR Imaging of Tumor and Tumorlike Lesions ofabdurrahmanNo ratings yet
- Investigation of ImmunotherapyDocument10 pagesInvestigation of Immunotherapyvoon_zhongNo ratings yet
- Ovarian Cancer Causes, Risk Factors, and PreventionDocument16 pagesOvarian Cancer Causes, Risk Factors, and PreventionSyafiqah HakimiNo ratings yet
- Epidemiology of Leukemia in Saudi ArabiaDocument19 pagesEpidemiology of Leukemia in Saudi ArabiaFaisal Al-SugairNo ratings yet
- Pancreatic Cancer Epidemiology and Risk FactorsDocument8 pagesPancreatic Cancer Epidemiology and Risk FactorsMARIA GABRIELA HERNANDEZ GONTOLNo ratings yet
- Benign Breast DiseaseDocument48 pagesBenign Breast DiseaseNabighah ZukriNo ratings yet
- Intra Individual Comparison of 18F PSMA1007 and 18F-FDG PETCT in The Evaluation of Patients With Prostate CancerDocument8 pagesIntra Individual Comparison of 18F PSMA1007 and 18F-FDG PETCT in The Evaluation of Patients With Prostate CancerJoaquín Escobar FloresNo ratings yet
- Dataset For Histopathological Reporting of Primary Invasive Cutaneous Squamous Cell Carcinoma and Regional Lymph NodesDocument57 pagesDataset For Histopathological Reporting of Primary Invasive Cutaneous Squamous Cell Carcinoma and Regional Lymph NodesMajid KhanNo ratings yet
- Cancer Survivor Speaks at Relay For Life CeremonyDocument1 pageCancer Survivor Speaks at Relay For Life CeremonycjtfhoaNo ratings yet
- ICD For OncologyDocument337 pagesICD For OncologytphivuongNo ratings yet
- Histological and Molecular Aspects of Oral Squamous Cell Carcinoma (Review)Document5 pagesHistological and Molecular Aspects of Oral Squamous Cell Carcinoma (Review)Yeni PuspitasariNo ratings yet
- Cancer Stem Cells Problems For TherapyDocument15 pagesCancer Stem Cells Problems For Therapyapi-162161895No ratings yet
- LeukemiaDocument5 pagesLeukemiaNourie BerawiNo ratings yet
- CS-PUB-LAB-1 Cervical Cytology Management Recommendations Explanatory GuideDocument11 pagesCS-PUB-LAB-1 Cervical Cytology Management Recommendations Explanatory GuideMc Coral100% (1)
- Epithelial Cell Abnormalities - GlandularDocument34 pagesEpithelial Cell Abnormalities - Glandularsarguss14No ratings yet