You might also like
- (2021) ISO 22341 (1st Edn)Document28 pages(2021) ISO 22341 (1st Edn)Dennis Mok100% (5)
- DIN EN 10293: April 2015Document21 pagesDIN EN 10293: April 2015My Dad My World50% (2)
- ALDO'S Global Omnichannel Imperative Group 8Document5 pagesALDO'S Global Omnichannel Imperative Group 8David RojasNo ratings yet
- The Beta-Blocker Story: Getting It RightFrom EverandThe Beta-Blocker Story: Getting It RightRating: 5 out of 5 stars5/5 (1)
- Smartphones - A Microeconomic AnalysisDocument27 pagesSmartphones - A Microeconomic AnalysisIshan ShahNo ratings yet
- Diseases of Bamboos in AsiaDocument228 pagesDiseases of Bamboos in AsiaDarío GarcíaNo ratings yet
- Chapter 7 (Adrenergic Antagonists)Document64 pagesChapter 7 (Adrenergic Antagonists)Aneeza AhmadNo ratings yet
- Beta Adrenergic Blockers: SympatholyticDocument12 pagesBeta Adrenergic Blockers: SympatholyticAbdullah asadNo ratings yet
- β - BlockersDocument12 pagesβ - Blockersmohavi8169No ratings yet
- Propranolol Introduced in 1963 Was A Therapeutic BreakthroughDocument5 pagesPropranolol Introduced in 1963 Was A Therapeutic BreakthroughOmkar Singh100% (1)
- 13 Beta Adrenoceptor BlockersDocument35 pages13 Beta Adrenoceptor BlockersanojanNo ratings yet
- Antihypertensive Agents: Ayman Khdair Ph.D. Pharmaceutical Sciences Wayne State University, Michigan, USADocument15 pagesAntihypertensive Agents: Ayman Khdair Ph.D. Pharmaceutical Sciences Wayne State University, Michigan, USAJalil HaddadinNo ratings yet
- Sympa T Holy TicsDocument30 pagesSympa T Holy TicsAhaisibwe GordonNo ratings yet
- PH 1.13:BETA Blockers: Dr. Lavakumar S Professor Dept of Pharmacology SssmcriDocument31 pagesPH 1.13:BETA Blockers: Dr. Lavakumar S Professor Dept of Pharmacology SssmcriBeena ShajimonNo ratings yet
- سموم نظري٤Document6 pagesسموم نظري٤مصطفى ابراهيم سعيدNo ratings yet
- Drugs of CvsDocument32 pagesDrugs of CvsAgus HaryantoNo ratings yet
- What Is AtenololDocument9 pagesWhat Is AtenololAbdelrhman AboodaNo ratings yet
- HTN Treatment DR - VishvasDocument46 pagesHTN Treatment DR - VishvasvishvasNo ratings yet
- Cardiovascular Pharmacology: Ana Sharmaine S. Uera, MD DR PJGMRMC Anesthesiology Department 1st Year ResidentDocument68 pagesCardiovascular Pharmacology: Ana Sharmaine S. Uera, MD DR PJGMRMC Anesthesiology Department 1st Year ResidentLalay CabanagNo ratings yet
- 2nd - Semester.lecture 3.1-Drugs Used in HypertensionDocument40 pages2nd - Semester.lecture 3.1-Drugs Used in HypertensionToader SilviaNo ratings yet
- Heart Failure Dr. VishvasDocument31 pagesHeart Failure Dr. VishvasvishvasNo ratings yet
- Beta Adrenergic Blockers ArvindDocument12 pagesBeta Adrenergic Blockers ArvindA2Z GyanNo ratings yet
- 3-11-2018 Beta Blocking DrugsDocument65 pages3-11-2018 Beta Blocking DrugsDharmendra GohilNo ratings yet
- Adrenergic AntagonistDocument29 pagesAdrenergic AntagonistAreesha ArifNo ratings yet
- Antiadrenergic Drugs - II 24.07.018 PDFDocument25 pagesAntiadrenergic Drugs - II 24.07.018 PDFHitesh karnNo ratings yet
- Summary of Product Characteristics: Concor 5 MG, Film-Coated Tablets Concor 10 MG, Film-Coated TabletsDocument12 pagesSummary of Product Characteristics: Concor 5 MG, Film-Coated Tablets Concor 10 MG, Film-Coated TabletsasdwasdNo ratings yet
- Lecture 1 antihypertensionSDSDocument7 pagesLecture 1 antihypertensionSDSSara AbbasNo ratings yet
- 6 SymaptholyticDocument48 pages6 SymaptholyticYoueel IbrahemNo ratings yet
- CVS AgentsDocument25 pagesCVS Agentsanon_925247980No ratings yet
- Drugs Without Positive Inotropic Effect Used in HFDocument12 pagesDrugs Without Positive Inotropic Effect Used in HFDana HamarshehNo ratings yet
- Adrenergic Blockers by Ms. MaidaDocument23 pagesAdrenergic Blockers by Ms. MaidaShimmering MoonNo ratings yet
- Atenolol: Atenolol Is A Beta Blocker MedicationDocument6 pagesAtenolol: Atenolol Is A Beta Blocker MedicationAbdelrhman AboodaNo ratings yet
- Sympa T Holy TicsDocument47 pagesSympa T Holy Ticsahmad tariqNo ratings yet
- CVS PHARM1pdf22Document57 pagesCVS PHARM1pdf22Dr. Hashibu SsekweyamaNo ratings yet
- Beta Blockers in HTNDocument69 pagesBeta Blockers in HTNMohammad Sadiq AzamNo ratings yet
- Controlled Hypotension: Moderator: DR V. Y. Srinivas Presenter: Dr. Ann Susan MathewDocument49 pagesControlled Hypotension: Moderator: DR V. Y. Srinivas Presenter: Dr. Ann Susan MathewAnn Susan MathewNo ratings yet
- Genxraver Girl Interrupted Usmle Step 2 Notes PDFDocument259 pagesGenxraver Girl Interrupted Usmle Step 2 Notes PDFughbuzzoffNo ratings yet
- Adrenergic Antagonists: Prepared by: Sevan Mahmod يسيردتلا رجفلا دهعم 07512491694Document64 pagesAdrenergic Antagonists: Prepared by: Sevan Mahmod يسيردتلا رجفلا دهعم 07512491694Ahmed MohamadNo ratings yet
- Beta-Blockers: Beta-Blocker Options Following Funding Changes To Betaloc CRDocument12 pagesBeta-Blockers: Beta-Blocker Options Following Funding Changes To Betaloc CRDewi Nurul SakinahNo ratings yet
- Pharmacology Reviewer FinalsDocument4 pagesPharmacology Reviewer FinalsCielo SanchezNo ratings yet
- New DrugsDocument2 pagesNew DrugsmayavargasNo ratings yet
- YogeshDocument49 pagesYogeshapi-3741769No ratings yet
- ANAESTHETICSDocument16 pagesANAESTHETICSAmbroseNo ratings yet
- Adrenergic Antagonist 2 (Propranolol)Document5 pagesAdrenergic Antagonist 2 (Propranolol)ziad shahinNo ratings yet
- 6 Beta Adrenergic BlockersDocument19 pages6 Beta Adrenergic Blockersmatchees-gone rogue100% (1)
- Pharmacology - Use of Beta-Blockers & Arbs in Cardiovascular Disease Treating HypertensionDocument5 pagesPharmacology - Use of Beta-Blockers & Arbs in Cardiovascular Disease Treating HypertensionDana20SNo ratings yet
- Beta Blockers: Dr. Mozna TalpurDocument12 pagesBeta Blockers: Dr. Mozna TalpurShahid HameedNo ratings yet
- SympatholyticsDocument46 pagesSympatholyticsHari Kamesh KiranNo ratings yet
- Beta BlockersDocument20 pagesBeta BlockersFarhat NaheedNo ratings yet
- Antiadrenergic 180630054321Document19 pagesAntiadrenergic 180630054321Dinam Gyatso AadHenmooNo ratings yet
- Central Nervous System DepressantsDocument11 pagesCentral Nervous System Depressantsاسامه عمر عثمانNo ratings yet
- Beta Adrenoceptor BlockersDocument30 pagesBeta Adrenoceptor BlockersShihab AlmoliukiNo ratings yet
- Case Study Number 1Document5 pagesCase Study Number 1Kevin Kyle RizarriNo ratings yet
- Cardio Lab MedsDocument11 pagesCardio Lab MedsDianne Erika MeguinesNo ratings yet
- Pharma Unit 8 - Anti - Adrenergic Drugs - 2 of 2Document21 pagesPharma Unit 8 - Anti - Adrenergic Drugs - 2 of 2MIbrahimNo ratings yet
- Anti Hypertensive 20191211Document35 pagesAnti Hypertensive 20191211helloitsmenadNo ratings yet
- Beta BlockersDocument3 pagesBeta BlockersWil LesterNo ratings yet
- Antihypertensive Drugs (2) - 092019Document33 pagesAntihypertensive Drugs (2) - 092019muntadhar5000No ratings yet
- NebivololDocument1 pageNebivololshaeNo ratings yet
- Beta-Blockers For Cardiovascular Conditions:: One Size Does Not Fit All PatientsDocument7 pagesBeta-Blockers For Cardiovascular Conditions:: One Size Does Not Fit All PatientsspalemaxNo ratings yet
- Adrenergic AntagonistDocument30 pagesAdrenergic AntagonistOmar AlaamNo ratings yet
- BB in HTN 2007Document69 pagesBB in HTN 2007doctopusNo ratings yet
- Adenoceptor Antagonist + Notes: DR - AltwijryDocument30 pagesAdenoceptor Antagonist + Notes: DR - Altwijryihsano_1No ratings yet
- Atrial Fibrillation A Simple Guide to The Condition, Treatment And Related DiseasesFrom EverandAtrial Fibrillation A Simple Guide to The Condition, Treatment And Related DiseasesRating: 4 out of 5 stars4/5 (1)
- DTI DirectoryDocument17 pagesDTI Directoryryan romeo perezNo ratings yet
- Qin Dynasty Unit 4Document30 pagesQin Dynasty Unit 4Amrit AdhikariNo ratings yet
- Eric PDFDocument5 pagesEric PDFAinah 16100% (1)
- Manual of NPN - To - PNP ConverterDocument2 pagesManual of NPN - To - PNP ConverterLaboratório de Ensaios de MotoresNo ratings yet
- E2 PTAct 2 9 1 DirectionsDocument2 pagesE2 PTAct 2 9 1 DirectionsAsad RiazNo ratings yet
- Silicon Conversion From Bamboo Leaf Silica by MagnDocument4 pagesSilicon Conversion From Bamboo Leaf Silica by MagnKim CantosNo ratings yet
- The Past Continuous TenseDocument4 pagesThe Past Continuous TenseMuhamadNevyNo ratings yet
- 25-06-22 - Incoming - JR Co Super Chaina Weekend Exam Syllabus ClarificationDocument1 page25-06-22 - Incoming - JR Co Super Chaina Weekend Exam Syllabus ClarificationJEE LEAKSNo ratings yet
- Amg1312-T10b 1Document300 pagesAmg1312-T10b 1brpnaidu2157No ratings yet
- HP G7000 Compaq Presario C700 Compal LA-3732P Spartan1.0 SchematicsDocument42 pagesHP G7000 Compaq Presario C700 Compal LA-3732P Spartan1.0 SchematicsLeonardo DiegoNo ratings yet
- ECE Lab Manual Requirements Sep 2021Document10 pagesECE Lab Manual Requirements Sep 2021supinya bieNo ratings yet
- Use in North America vs. Europe: Outdoor SpaceDocument27 pagesUse in North America vs. Europe: Outdoor SpaceDB FasikaNo ratings yet
- Learners' Names: Input Data Sheet For SHS E-Class RecordDocument23 pagesLearners' Names: Input Data Sheet For SHS E-Class RecordChristine Joy MaapoyNo ratings yet
- Gillies (1995) Bartók Analysis and AuthenticityDocument10 pagesGillies (1995) Bartók Analysis and AuthenticityIma Bage100% (1)
- Lavadora - WF165Document98 pagesLavadora - WF165Jose AltuveNo ratings yet
- Curriculum Map Math 10 1 (Recovered)Document6 pagesCurriculum Map Math 10 1 (Recovered)Rocel Mae L. GambaNo ratings yet
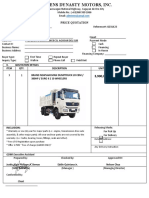
- Price Quotation Shacman H3000 Dump TruckDocument1 pagePrice Quotation Shacman H3000 Dump TruckJustin BernasNo ratings yet
- 20462C ENU StudentHandbookDocument430 pages20462C ENU StudentHandbookGalapagos GeorgeNo ratings yet
- @enmagazine 2019-01-01 Teen Breathe PDFDocument68 pages@enmagazine 2019-01-01 Teen Breathe PDFSheila Jamil100% (2)
- Syllabus 4th SemDocument3 pagesSyllabus 4th SemPrianca PrathapNo ratings yet
- UK Garments Importer - PDF - Clothing - T ShirtDocument21 pagesUK Garments Importer - PDF - Clothing - T ShirtKishan ZatakiyaNo ratings yet
- Theatelus-The Five Platonic Solids 400 BDocument13 pagesTheatelus-The Five Platonic Solids 400 Bapi-340711178No ratings yet
- Final Exam On EpistemologyDocument2 pagesFinal Exam On EpistemologyChristian PagayananNo ratings yet
- User's Manual of Haiwell IoT Cloud HMIDocument39 pagesUser's Manual of Haiwell IoT Cloud HMIRolando NuñezNo ratings yet
- 1 - Ansell Edge - Complete 1023Document44 pages1 - Ansell Edge - Complete 1023Ben5 Farm IIINo ratings yet