You might also like
- idm-22030319584Document51 pagesidm-22030319584Harini KarthikeyanNo ratings yet
- Diabetes in Pregnancy - BibDocument54 pagesDiabetes in Pregnancy - BibNadhrah zulkifliNo ratings yet
- Art-Rol Del Ejercicio para Reducir La DM GestacionalDocument13 pagesArt-Rol Del Ejercicio para Reducir La DM GestacionalPaula RangelNo ratings yet
- DIABETES MELLITUS HandoutDocument11 pagesDIABETES MELLITUS HandoutYurika KinoshitaNo ratings yet
- DM in PregnancyDocument35 pagesDM in Pregnancyapule geraldhumbleNo ratings yet
- Nutricare in Diabetes With Special ConditionsDocument40 pagesNutricare in Diabetes With Special ConditionsNudrat KhanNo ratings yet
- MEDICAL COMPLICATIONS OF PREGNANCY ModuleDocument12 pagesMEDICAL COMPLICATIONS OF PREGNANCY ModuleWynjoy NebresNo ratings yet
- DM in PregDocument32 pagesDM in Pregbryanpei23No ratings yet
- Gestational DiabetesDocument35 pagesGestational DiabetesAnnakay HudsonNo ratings yet
- Diabetes in PregnancyDocument66 pagesDiabetes in PregnancySuhashis MukherjeeNo ratings yet
- Diabetes in PrgenancyDocument36 pagesDiabetes in Prgenancynita meliasariNo ratings yet
- 56 Diabetes in Pregnancy - OBS16Document32 pages56 Diabetes in Pregnancy - OBS16collinsmagNo ratings yet
- Infant of A Diabetic MotherDocument17 pagesInfant of A Diabetic MotherLovina Falendini AndriNo ratings yet
- Gestational Diabetes Mellitus - : One Disease Two Lives at StakeDocument31 pagesGestational Diabetes Mellitus - : One Disease Two Lives at StakeSadia YousafNo ratings yet
- dminpregnancy-201109140122 (1)Document76 pagesdminpregnancy-201109140122 (1)EndaleNo ratings yet
- Ayesha Khatun 15A, Topic - Diabetes and PregnancyDocument40 pagesAyesha Khatun 15A, Topic - Diabetes and PregnancyAyesha KhatunNo ratings yet
- IDM Infants of Diabetic MothersDocument80 pagesIDM Infants of Diabetic MothersManor AlienNo ratings yet
- Gestational Diabetus MellitusDocument28 pagesGestational Diabetus MellitusSanthosh.S.U100% (1)
- Complicated Midwifery - 1Document28 pagesComplicated Midwifery - 1nafisatmuhammed452No ratings yet
- Childhood Obesity, Insulin Resistance, and Risk of Type 2 DiabetesDocument28 pagesChildhood Obesity, Insulin Resistance, and Risk of Type 2 Diabetesmahdi arif prasetyaNo ratings yet
- Gestational Diabetes: Key PointsDocument5 pagesGestational Diabetes: Key PointsMayra PereiraNo ratings yet
- Inpatient Glycemic ManagementDocument13 pagesInpatient Glycemic Managementmiss betawiNo ratings yet
- Gestational Diabetus MellitusDocument28 pagesGestational Diabetus MellitusSanthosh.S.UNo ratings yet
- Congenital Abnormalities IDMDocument9 pagesCongenital Abnormalities IDMkatskoufNo ratings yet
- Gestational Diabetes Screening in AustraliaDocument9 pagesGestational Diabetes Screening in AustraliaRaniMSinghNo ratings yet
- Congenital Abnormalities in The Infant of A Diabetic Mother: Practice GapDocument9 pagesCongenital Abnormalities in The Infant of A Diabetic Mother: Practice GapIgnacio Andres Correa KarstulovicNo ratings yet
- Lesson#7 - Diabetes MellitusDocument22 pagesLesson#7 - Diabetes MellitusKyle Ethan De la RiarteNo ratings yet
- Complications Delivery InformationDocument22 pagesComplications Delivery Informationdiabetes asiaNo ratings yet
- Children's Diabetes: Causes, Symptoms and TreatmentDocument52 pagesChildren's Diabetes: Causes, Symptoms and TreatmentAmmar AlnajjarNo ratings yet
- Gestational Diabetes MellitusDocument31 pagesGestational Diabetes MellitusLidya BintangNo ratings yet
- Diabetes in Pregnancy: DR Richard A GreeneDocument19 pagesDiabetes in Pregnancy: DR Richard A GreeneJayanti Ika siwiNo ratings yet
- Diabetes in PregnancyDocument88 pagesDiabetes in PregnancyKathleenZunigaNo ratings yet
- Newborn of A Diabetic Melitus MotherDocument22 pagesNewborn of A Diabetic Melitus MotherDennis MiritiNo ratings yet
- Paeda DMDocument38 pagesPaeda DMAmanuel LemiNo ratings yet
- Gestational Diabetes Mellitus: Managing Two Lives at RiskDocument54 pagesGestational Diabetes Mellitus: Managing Two Lives at RiskAnjali LimbuNo ratings yet
- Tipos de Diabetes - Diabetes MonogenicaDocument27 pagesTipos de Diabetes - Diabetes MonogenicaSara AmorimNo ratings yet
- Diabetes and Pregnancy: Syamel Muhammad, Dr. Spog K.OnkDocument41 pagesDiabetes and Pregnancy: Syamel Muhammad, Dr. Spog K.Onkyessy tamaraNo ratings yet
- Managing Gestational Diabetes and MacrosomiaDocument30 pagesManaging Gestational Diabetes and MacrosomiaCharlz ZipaganNo ratings yet
- Managing complications of infants of diabetic mothersDocument60 pagesManaging complications of infants of diabetic mothersEman KhammasNo ratings yet
- لقطة شاشة ٢٠٢٤-٠٢-٢٦ في ٣.٠٨.٢٩ مDocument32 pagesلقطة شاشة ٢٠٢٤-٠٢-٢٦ في ٣.٠٨.٢٩ مali1alio11aaNo ratings yet
- GDIABETUS MELITUS EyobDocument60 pagesGDIABETUS MELITUS Eyobm.pfortress.ojNo ratings yet
- Diabetus Mellitus: Dr. Fawzi Radi F.R.C.O.GDocument19 pagesDiabetus Mellitus: Dr. Fawzi Radi F.R.C.O.GCrissLaraNo ratings yet
- Presenter: Dr. P. Usha Rani Resident, ASRAMS, EluruDocument60 pagesPresenter: Dr. P. Usha Rani Resident, ASRAMS, EluruDivya Rekha KolliNo ratings yet
- Maternal Carbohydrate Metabolism During Pregnancy and GDMDocument37 pagesMaternal Carbohydrate Metabolism During Pregnancy and GDMCrifer RondonuwuNo ratings yet
- GDMDocument26 pagesGDMListon OtienoNo ratings yet
- Diabetes Mellitus: Nestan BostoganashviliDocument31 pagesDiabetes Mellitus: Nestan BostoganashviliAlireza FarhadiehNo ratings yet
- Recent Advances in Management of Gestational Diabetes and Pre-EclampsiaDocument36 pagesRecent Advances in Management of Gestational Diabetes and Pre-EclampsiaSyed Zahed AliNo ratings yet
- Diabetes in Pregnancy: Supervisor: DR Rathimalar By: DR Ashwini Arumugam & DR Laily MokhtarDocument21 pagesDiabetes in Pregnancy: Supervisor: DR Rathimalar By: DR Ashwini Arumugam & DR Laily MokhtarHarleyquinn96 DrNo ratings yet
- Pre-Gestational Cardiovascular Conditions in PregnancyDocument29 pagesPre-Gestational Cardiovascular Conditions in PregnancyVyklyn TestaNo ratings yet
- Milk and Metabolic SyndromeDocument10 pagesMilk and Metabolic SyndromeCamilla MendesNo ratings yet
- Fdocuments - in Metabolic Disorders of Pregnancy Gestational Disorders of Pregnancy GestationalDocument42 pagesFdocuments - in Metabolic Disorders of Pregnancy Gestational Disorders of Pregnancy GestationalSoniya100% (1)
- Gestational Diabetes: Dr. Oyeyiola Oyebode Registrar Obstetrics and Gynaecology Ola Catholic Hospital, Oluyoro IbadanDocument40 pagesGestational Diabetes: Dr. Oyeyiola Oyebode Registrar Obstetrics and Gynaecology Ola Catholic Hospital, Oluyoro Ibadanoyebode oyeyiolaNo ratings yet
- Diabetes Mellitus & Pregnancy by D.a.mehtaDocument31 pagesDiabetes Mellitus & Pregnancy by D.a.mehtadr.d.a.mehta11No ratings yet
- Pediatric DMDocument39 pagesPediatric DMmy Lord JesusNo ratings yet
- sullivan1998 ເອກະສານອ້າງອີງ ຈາກ ວິທີວິທະຍາDocument10 pagessullivan1998 ເອກະສານອ້າງອີງ ຈາກ ວິທີວິທະຍາKab Zuag HaamNo ratings yet
- Diabetes Mellitus: Prepared by Divya Bhusal B.SC - Nursing 3 YearDocument43 pagesDiabetes Mellitus: Prepared by Divya Bhusal B.SC - Nursing 3 YearSristi LamsalNo ratings yet
- Infants of Diabetic MothersDocument19 pagesInfants of Diabetic MothersGaby AldamaNo ratings yet
- Intrapartum DM Management: By: DRDocument38 pagesIntrapartum DM Management: By: DRYohannis AsefaNo ratings yet
- Emergencies in Diabetes: Diagnosis, Management and PreventionFrom EverandEmergencies in Diabetes: Diagnosis, Management and PreventionNo ratings yet
- Conquering Diabetes: Fenugreek Success in Regulating Blood Sugar LevelsFrom EverandConquering Diabetes: Fenugreek Success in Regulating Blood Sugar LevelsNo ratings yet
- Situs JurnalDocument1 pageSitus JurnalBayna Lestari LubisNo ratings yet
- Daftar Kelulusan MCQSCBT Periode November 2018Document58 pagesDaftar Kelulusan MCQSCBT Periode November 2018larasNo ratings yet
- 6807 DikonversiDocument10 pages6807 DikonversiBayna Lestari LubisNo ratings yet
- AJOG2003 188-DikonversiDocument8 pagesAJOG2003 188-DikonversiBayna Lestari LubisNo ratings yet
- Magnesium Sulfat DikonversiDocument23 pagesMagnesium Sulfat DikonversiBayna Lestari LubisNo ratings yet
- Foetal Macrosomia and Foetal-Maternal Outcomes at Birth: Sahruh Turkmen, Simona Johansson, and Marju DahmounDocument9 pagesFoetal Macrosomia and Foetal-Maternal Outcomes at Birth: Sahruh Turkmen, Simona Johansson, and Marju DahmounBayna Lestari LubisNo ratings yet
- Foetal Macrosomia and Foetal-Maternal Outcomes at Birth: Sahruh Turkmen, Simona Johansson, and Marju DahmounDocument9 pagesFoetal Macrosomia and Foetal-Maternal Outcomes at Birth: Sahruh Turkmen, Simona Johansson, and Marju DahmounBayna Lestari LubisNo ratings yet
- Hubungan Antara Endometriosis Fertility Index (Efi) Dan Keberhasilan Fertilisasi in Vitro (Fiv)Document9 pagesHubungan Antara Endometriosis Fertility Index (Efi) Dan Keberhasilan Fertilisasi in Vitro (Fiv)Bayna Lestari LubisNo ratings yet
- Early Predictors For Hypertensive Disorders of Pregnancy in Developing CountriesDocument12 pagesEarly Predictors For Hypertensive Disorders of Pregnancy in Developing CountriesBayna Lestari LubisNo ratings yet
- EngDocument134 pagesEngAgrim KhatryNo ratings yet
- DCHHVDZ BJGFJ NHJKGFG BKKMNGFF Bhukmb MJGFGBDocument1 pageDCHHVDZ BJGFJ NHJKGFG BKKMNGFF Bhukmb MJGFGBBayna Lestari LubisNo ratings yet
- Lampiran E Master Tabel Binatang PeliharaanDocument1 pageLampiran E Master Tabel Binatang PeliharaanBayna Lestari LubisNo ratings yet
- NO. Nama Umur Tempat Tinggal DiagnosaDocument13 pagesNO. Nama Umur Tempat Tinggal DiagnosaBayna Lestari LubisNo ratings yet
- NO. Nama Umur Tempat Tinggal DiagnosaDocument9 pagesNO. Nama Umur Tempat Tinggal DiagnosaBayna Lestari LubisNo ratings yet
- EngDocument134 pagesEngAgrim KhatryNo ratings yet
- Breastfeeding and The Use of Human Milk: An Analysis of The American Academy of Pediatrics 2012 Breastfeeding Policy StatementDocument2 pagesBreastfeeding and The Use of Human Milk: An Analysis of The American Academy of Pediatrics 2012 Breastfeeding Policy StatementBayna Lestari LubisNo ratings yet
- Cir625 PDFDocument14 pagesCir625 PDFAnindita Candra DewiNo ratings yet
- AMCV Mop Up Allotment ResultsDocument73 pagesAMCV Mop Up Allotment Resultsbache saiNo ratings yet
- Consensus ETON 1Document7 pagesConsensus ETON 1satyagraha84No ratings yet
- Strong Letter of Recommendation for Radiology ResidencyDocument1 pageStrong Letter of Recommendation for Radiology Residencydrsanjeev15No ratings yet
- Aub Physical Examination of UrineDocument3 pagesAub Physical Examination of UrineKristine BaringNo ratings yet
- NURSING CARE FOR LABOR PAINDocument5 pagesNURSING CARE FOR LABOR PAINMarco VillanuevaNo ratings yet
- MELD-Plus Wiki Nov 24 2019Document3 pagesMELD-Plus Wiki Nov 24 2019UKNo ratings yet
- C This Is Only A Summary.: Important Questions Answers Why This MattersDocument8 pagesC This Is Only A Summary.: Important Questions Answers Why This MattersChris DuffnerNo ratings yet
- Abnormal Expulsive Forces of The UterusDocument2 pagesAbnormal Expulsive Forces of The UterusSayyeda niha AkhtarNo ratings yet
- RX Ileus Meconial CFDocument1 pageRX Ileus Meconial CFRaluca MosoiaNo ratings yet
- Mechanical Properties of Resilon and Gutta-Percha Under Flexural StressesDocument1 pageMechanical Properties of Resilon and Gutta-Percha Under Flexural Stressesaay18bdsNo ratings yet
- Test Bank For Maternity and Womens Health Care 12th Edition Deitra Leonard Lowdermilk Shannon e Perry Mary Catherine Cashion Kathryn Rhodes Alden Ellen OlshanskyDocument9 pagesTest Bank For Maternity and Womens Health Care 12th Edition Deitra Leonard Lowdermilk Shannon e Perry Mary Catherine Cashion Kathryn Rhodes Alden Ellen Olshanskysubitodomesticcz70o3No ratings yet
- Preterm Labour: Pembimbing: Dr. Andriana Kumala Dewi, SP - OGDocument33 pagesPreterm Labour: Pembimbing: Dr. Andriana Kumala Dewi, SP - OGJovian LutfiNo ratings yet
- Reading 8Document8 pagesReading 8nhung phanNo ratings yet
- NEONATAL JAUNDICE: CAUSES, RISK FACTORS AND MANAGEMENTDocument23 pagesNEONATAL JAUNDICE: CAUSES, RISK FACTORS AND MANAGEMENTAsad M AminNo ratings yet
- MIRA2011 Athensadv ProgramDocument64 pagesMIRA2011 Athensadv ProgramMIRA 2011 ATHENSNo ratings yet
- Radiology approach and controversies in small bowel obstructionDocument20 pagesRadiology approach and controversies in small bowel obstructionherfikaNo ratings yet
- VSM SecureDocument0 pagesVSM SecurekariolitsaNo ratings yet
- Elderly PrimiDocument7 pagesElderly PrimiAnnapurna Dangeti67% (3)
- Poroma of The Hip and ButtockDocument3 pagesPoroma of The Hip and ButtockDeba P SarmaNo ratings yet
- ATOTW 136 Major Haemorrhage Part 1 2009Document6 pagesATOTW 136 Major Haemorrhage Part 1 2009viaereaNo ratings yet
- Malignant Hyperthermia AlgorithmDocument1 pageMalignant Hyperthermia AlgorithmCesar David CaceresNo ratings yet
- Exploratory Laparotomy PDFDocument8 pagesExploratory Laparotomy PDFFadhil ShalihNo ratings yet
- An Analysis of A Film Gifted HandsDocument9 pagesAn Analysis of A Film Gifted Handscitra indah syaputri100% (1)
- Circumcision OverviewDocument3 pagesCircumcision Overviewcsalas31No ratings yet
- Maxicare List of PhysiciansDocument3,952 pagesMaxicare List of PhysiciansEdrian Boado75% (4)
- Roles of Barangay Health WorkersDocument13 pagesRoles of Barangay Health WorkersFret Ramirez Coronia RN71% (7)
- Dialysis in ChildrenDocument15 pagesDialysis in ChildrenMani VachaganNo ratings yet
- Kerra Resume DH Weebly 2Document1 pageKerra Resume DH Weebly 2api-413075749No ratings yet
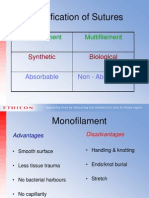
- Classification of Sutures: Monofilament MultifilamentDocument17 pagesClassification of Sutures: Monofilament Multifilamentlina_m354No ratings yet
- Soal Ujian R2 FixedDocument9 pagesSoal Ujian R2 Fixedprakoso jatiNo ratings yet