You might also like
- Ophthalmology Review Manual 2nd EditionDocument538 pagesOphthalmology Review Manual 2nd EditionAnonymous 4OnqyBErNo ratings yet
- Analysis of Survival Data - LN - D Zhang - 05Document264 pagesAnalysis of Survival Data - LN - D Zhang - 05mirceacomanro2740100% (1)
- IeltsDocument65 pagesIeltskitten_alina92% (13)
- Basics of Biostatistics PDFDocument31 pagesBasics of Biostatistics PDFDrAnisha PatelNo ratings yet
- Congenital Abnormalities in The Infant of A Diabetic Mother: Practice GapDocument9 pagesCongenital Abnormalities in The Infant of A Diabetic Mother: Practice GapIgnacio Andres Correa KarstulovicNo ratings yet
- Neoreviews 042022cmerev00036Document12 pagesNeoreviews 042022cmerev00036Agnimitra ChoudhuryNo ratings yet
- Review of Pathophysiology and Management of Diabetes in PregnancyDocument13 pagesReview of Pathophysiology and Management of Diabetes in Pregnancyfelipe_duran_scribdNo ratings yet
- Diabetes in PrgenancyDocument36 pagesDiabetes in Prgenancynita meliasariNo ratings yet
- 1 s2.0 S2058534919301519 MainDocument5 pages1 s2.0 S2058534919301519 MainjhuyNo ratings yet
- Disbetes Obs PDFDocument18 pagesDisbetes Obs PDFdhruvNo ratings yet
- Gestational Diabetes Mellitus Pathogenesis and ComplicationsDocument56 pagesGestational Diabetes Mellitus Pathogenesis and ComplicationsBayna Lestari LubisNo ratings yet
- Saudi J Med Med Sci 2014 2 3 151 156Document6 pagesSaudi J Med Med Sci 2014 2 3 151 156Manor AlienNo ratings yet
- DIABETES MELLITUS HandoutDocument11 pagesDIABETES MELLITUS HandoutYurika KinoshitaNo ratings yet
- Infants of Diabetic Mothers: Back To BasicsDocument3 pagesInfants of Diabetic Mothers: Back To BasicskiloNo ratings yet
- Gestational Diabetes: Key PointsDocument5 pagesGestational Diabetes: Key PointsMayra PereiraNo ratings yet
- Bowe, 2018)Document7 pagesBowe, 2018)Mayra PereiraNo ratings yet
- New Concepts in Diabetic EmbryopathyDocument35 pagesNew Concepts in Diabetic EmbryopathyGabyliz Gonzalez CastilloNo ratings yet
- WWW Ncbi NLM Nih GovDocument10 pagesWWW Ncbi NLM Nih GovJumrah KhumairahNo ratings yet
- 2021 Bastidas Uriel de La Hoz Romero Pre Proof Perinatal Outcomes Diagnosis DM Systematic Review Meta-AnalysisDocument8 pages2021 Bastidas Uriel de La Hoz Romero Pre Proof Perinatal Outcomes Diagnosis DM Systematic Review Meta-AnalysisMiguelEstebanBaqueroAcuñaNo ratings yet
- Febriyanti M. AdamDocument23 pagesFebriyanti M. AdamRinda UnoNo ratings yet
- Insulin Use in Pregnancy: An UpdateDocument6 pagesInsulin Use in Pregnancy: An UpdateZaniru Raúl Marín MartínezNo ratings yet
- Diabetes Mellitus and Pregnancy: Chapter OutlineDocument21 pagesDiabetes Mellitus and Pregnancy: Chapter OutlineqalbiNo ratings yet
- 4 Gestational Diabetes MellitusDocument12 pages4 Gestational Diabetes MellitusAnonymous tgLZ9uvXsNo ratings yet
- Diabetes Mellitus GestationalDocument19 pagesDiabetes Mellitus GestationalYosefin RatnaningtyasNo ratings yet
- Gestational Diabetes Mellitus: Science in MedicineDocument7 pagesGestational Diabetes Mellitus: Science in MedicinerizqarrNo ratings yet
- Journal GAJOMSDocument6 pagesJournal GAJOMSmade dharmaNo ratings yet
- Referat PDGMDocument31 pagesReferat PDGMFazlurrahmanNo ratings yet
- Gestational Diabetes Mellitus Is Associated With Adverse Outcomes in Twin PregnanciesDocument8 pagesGestational Diabetes Mellitus Is Associated With Adverse Outcomes in Twin PregnanciesDwi OktaviliaNo ratings yet
- Correlations Between Parameters of Glycaemic Variability and Foetal Growth Neonatal Hypoglycaemia and Hyperbilirubinemia in Women With Gestational diabetesPLoS ONEDocument14 pagesCorrelations Between Parameters of Glycaemic Variability and Foetal Growth Neonatal Hypoglycaemia and Hyperbilirubinemia in Women With Gestational diabetesPLoS ONEVicente Fasce OlmosNo ratings yet
- Gestational Diabetes Mellitus: Thomas A. Buchanan, Anny H. XiangDocument8 pagesGestational Diabetes Mellitus: Thomas A. Buchanan, Anny H. Xiangalen walkerNo ratings yet
- Cornejo 2021Document15 pagesCornejo 2021Rohan PandeyNo ratings yet
- Infants of Diabetic MothersDocument19 pagesInfants of Diabetic MothersGaby AldamaNo ratings yet
- Art-Rol Del Ejercicio para Reducir La DM GestacionalDocument13 pagesArt-Rol Del Ejercicio para Reducir La DM GestacionalPaula RangelNo ratings yet
- HAPO Study Examines Associations Between Maternal Glycemia and Adverse Pregnancy OutcomesDocument9 pagesHAPO Study Examines Associations Between Maternal Glycemia and Adverse Pregnancy OutcomesEstefania GutierrezNo ratings yet
- Preexisting Diabetes in Pregnancy ReviewDocument21 pagesPreexisting Diabetes in Pregnancy Reviewsabela afrilaNo ratings yet
- Gestational Diabetes Mellitus Acog CopDocument8 pagesGestational Diabetes Mellitus Acog CopAndrea Sandoval OteroNo ratings yet
- Prenatal Diagnosis - 2020 - Murray - Short and Long Term Outcomes of Gestational Diabetes and Its Treatment On FetalDocument7 pagesPrenatal Diagnosis - 2020 - Murray - Short and Long Term Outcomes of Gestational Diabetes and Its Treatment On FetalVicente Fasce OlmosNo ratings yet
- ACOG Practice Bulletin No137 PDFDocument11 pagesACOG Practice Bulletin No137 PDFRodrigo Pérez CuelloNo ratings yet
- Gestational Diabetes Mellitus: Nature Reviews Disease Primers July 2019Document20 pagesGestational Diabetes Mellitus: Nature Reviews Disease Primers July 2019Mohammed RickyNo ratings yet
- Consequences of Gestational and Pregestational Diabetes On Placental Function and Birth WeightDocument8 pagesConsequences of Gestational and Pregestational Diabetes On Placental Function and Birth WeightannisaNo ratings yet
- Diabetes Ada 2020 PDFDocument10 pagesDiabetes Ada 2020 PDFOrlando CuellarNo ratings yet
- The Elusive Diagnosis of Gestational Diabetes: Guest EditorialDocument4 pagesThe Elusive Diagnosis of Gestational Diabetes: Guest EditorialSarly FebrianaNo ratings yet
- Animal Model For Gestational DiabetesDocument14 pagesAnimal Model For Gestational DiabetesAnushka DhandeNo ratings yet
- FattyliverinpregnancyDocument8 pagesFattyliverinpregnancyJulieta Urano DelgadoNo ratings yet
- Infants of Diabetic Mothers ComplicationsDocument19 pagesInfants of Diabetic Mothers ComplicationsYong Kui ChooNo ratings yet
- Neonatal HypoglycemiaDocument19 pagesNeonatal Hypoglycemiasylviaoctaviany13No ratings yet
- Management of Preexisting Diabetes in Pregnancy 2019Document9 pagesManagement of Preexisting Diabetes in Pregnancy 2019Residentes GinecologíaNo ratings yet
- Diabetes in Pregnancy: Screening, Management, and OutcomesDocument7 pagesDiabetes in Pregnancy: Screening, Management, and Outcomeseka putri nur azizahNo ratings yet
- Inpatient Glycemic ManagementDocument13 pagesInpatient Glycemic Managementmiss betawiNo ratings yet
- Gestational Diabetes Mellitus (GDM) : Current Concept and A Short ReviewDocument1 pageGestational Diabetes Mellitus (GDM) : Current Concept and A Short ReviewTimothy Ho IINo ratings yet
- Type1Diabetesinpregnancy: David R. Mccance,, Claire CaseyDocument15 pagesType1Diabetesinpregnancy: David R. Mccance,, Claire Caseyjose ricardo escalante perezNo ratings yet
- Gestational Diabetes Mellitus: Risks and Management During and After PregnancyDocument11 pagesGestational Diabetes Mellitus: Risks and Management During and After PregnancyViki G PNo ratings yet
- Placental Metabolic Derangements and Fetal Complications in Gestational DiabetesDocument11 pagesPlacental Metabolic Derangements and Fetal Complications in Gestational Diabetesbalachandiran manoharanNo ratings yet
- International Journal of Diabetes MellitusDocument7 pagesInternational Journal of Diabetes MellitusTiti IndasariNo ratings yet
- Diabetes Mellitus and Fetal DistressDocument7 pagesDiabetes Mellitus and Fetal DistressSuci ArNo ratings yet
- Gestational Diabetes Mellitus: New Diagnostic CriteriaDocument7 pagesGestational Diabetes Mellitus: New Diagnostic CriteriaRambuNo ratings yet
- Jurnal DM GestasionalDocument18 pagesJurnal DM GestasionalEchi DesnawatiNo ratings yet
- Malformaciones Por Diabetes y ObesidadDocument8 pagesMalformaciones Por Diabetes y ObesidadKaren LeónNo ratings yet
- Gestational DiabetesDocument35 pagesGestational DiabetesAnnakay HudsonNo ratings yet
- Gestational Diabetes Screening in AustraliaDocument9 pagesGestational Diabetes Screening in AustraliaRaniMSinghNo ratings yet
- Prediabetes: A Fundamental Text: Pathophysiology, Complications, Management & ReversalFrom EverandPrediabetes: A Fundamental Text: Pathophysiology, Complications, Management & ReversalNo ratings yet
- Conquering Diabetes: Fenugreek Success in Regulating Blood Sugar LevelsFrom EverandConquering Diabetes: Fenugreek Success in Regulating Blood Sugar LevelsNo ratings yet
- The Ideal Gestational Diabetes Diet Cookbook; The Superb Diet Guide For Healthy Pregnancy And Baby With Meal Plan And Nutritious RecipesFrom EverandThe Ideal Gestational Diabetes Diet Cookbook; The Superb Diet Guide For Healthy Pregnancy And Baby With Meal Plan And Nutritious RecipesNo ratings yet
- EUCAST V - 9.0 - Breakpoint - Tables PDFDocument100 pagesEUCAST V - 9.0 - Breakpoint - Tables PDFRicardo Ariel GianeciniNo ratings yet
- ResearcfhSleep DeprivationDocument36 pagesResearcfhSleep DeprivationDonna CatantanNo ratings yet
- VBMC Heparin Protocol FINAL May2004Document3 pagesVBMC Heparin Protocol FINAL May2004Pharmacy OneSource100% (1)
- Memory Reconsolidation Applied - Calm Your Past To Live Your FutureDocument177 pagesMemory Reconsolidation Applied - Calm Your Past To Live Your Futureiskieh100% (7)
- Anxiety Disorders: Powerpoint Lecture Notes PresentationDocument43 pagesAnxiety Disorders: Powerpoint Lecture Notes PresentationErsido SamuelNo ratings yet
- Galactocele Is A Benign Breast Tumor of The Mammary Gland Which Is More Prevalent During Pregnancy or LactationDocument4 pagesGalactocele Is A Benign Breast Tumor of The Mammary Gland Which Is More Prevalent During Pregnancy or LactationTheQueensafa90No ratings yet
- Childhood Atopic Dermatitis: Current Developments, Treatment Approaches, and Future ExpectationsDocument22 pagesChildhood Atopic Dermatitis: Current Developments, Treatment Approaches, and Future Expectationsyenny handayani sihiteNo ratings yet
- Music Therapy For Non - Alzheimer's Disease Dementia: A Systematic ReviewDocument9 pagesMusic Therapy For Non - Alzheimer's Disease Dementia: A Systematic ReviewMaría DiazNo ratings yet
- HepatomegalyDocument1 pageHepatomegalywounded86100% (1)
- Mini Case Study WeeblyDocument5 pagesMini Case Study Weeblyapi-270446591No ratings yet
- Quality of Life After Functional Endoscopic Sinus Surgery in Patients With Chronic RhinosinusitisDocument15 pagesQuality of Life After Functional Endoscopic Sinus Surgery in Patients With Chronic RhinosinusitisNarendraNo ratings yet
- 15 Zeolite Uses & Benefits (Incl. Detox) + Side Effects - SelfhackedDocument19 pages15 Zeolite Uses & Benefits (Incl. Detox) + Side Effects - SelfhackedtsolakidesmedNo ratings yet
- PHD Thesis in Prevalence of AsthmaDocument7 pagesPHD Thesis in Prevalence of Asthmabk3q07k5100% (1)
- Document - Isk ..Document8 pagesDocument - Isk ..Karyn GloriaNo ratings yet
- Nursing Care Plan for Urinary Tract Infection (UTIDocument19 pagesNursing Care Plan for Urinary Tract Infection (UTIYudistiro Adi Nugroho100% (1)
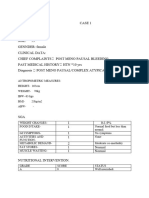
- Case 1Document7 pagesCase 1bsc.clinicalnutrition2018No ratings yet
- AAO - External Disease and CorneaDocument19 pagesAAO - External Disease and CorneaJohn Paul VillaflorNo ratings yet
- Corpus Alienum VaginaeDocument3 pagesCorpus Alienum VaginaeIntan PermataNo ratings yet
- Paget Disease, Fibrous Dysplasia, Osteosarcoma DiffrentiationDocument3 pagesPaget Disease, Fibrous Dysplasia, Osteosarcoma Diffrentiationreason131No ratings yet
- Treatment For Spider Veins On LegsDocument3 pagesTreatment For Spider Veins On LegsZackNo ratings yet
- Mhps-Ts Newsletter: MHPS Technical Services CorporationDocument21 pagesMhps-Ts Newsletter: MHPS Technical Services Corporationjonel.javierNo ratings yet
- Avhad (2020), Comparison of Effectiveness of Chlorine Dioxide Mouthwash and Chlorhexidine Gluconate Mouthwash in Reduction of Oral Viral Load in Patients With COVID-19Document6 pagesAvhad (2020), Comparison of Effectiveness of Chlorine Dioxide Mouthwash and Chlorhexidine Gluconate Mouthwash in Reduction of Oral Viral Load in Patients With COVID-19Phuong ThaoNo ratings yet
- New Patient Nutrition Assessment Form: (Person 1)Document12 pagesNew Patient Nutrition Assessment Form: (Person 1)Ayesha KhanNo ratings yet
- SynapsesDocument46 pagesSynapseshan abuur ahmedNo ratings yet
- JR Science Quiz 19-20 Class VI - VIIIDocument43 pagesJR Science Quiz 19-20 Class VI - VIIIDAVV IQACNo ratings yet
- Theoretical Framework - GiannaDocument2 pagesTheoretical Framework - GiannaAnne MarielNo ratings yet