You might also like
- Emergency Hypertension (Herbesser Injection)Document18 pagesEmergency Hypertension (Herbesser Injection)suho exoNo ratings yet
- Hipertensi EmergencyDocument31 pagesHipertensi Emergencysar tikaNo ratings yet
- Managing Hypertensive CrisesDocument31 pagesManaging Hypertensive CrisesAmanda DavisNo ratings yet
- ShockDocument39 pagesShockCut Ristina OlviaNo ratings yet
- Inotropes and Vasopressors: Definition RecapDocument2 pagesInotropes and Vasopressors: Definition RecapThistell ThistleNo ratings yet
- AkshayDocument35 pagesAkshaySheryl VarshneyNo ratings yet
- Hypertension: A Major Risk Factor for Stroke and Heart DiseaseDocument43 pagesHypertension: A Major Risk Factor for Stroke and Heart DiseaseBobby WidiastomoNo ratings yet
- Management of HypertensionDocument64 pagesManagement of HypertensionAnonymous h0DxuJTNo ratings yet
- Hypertensive Crisis ManagementDocument27 pagesHypertensive Crisis ManagementDian Puspa100% (1)
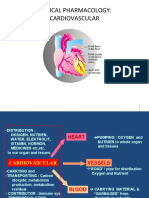
- CLINICAL PHARMACOLOGY OF CARDIOVASCULAR DRUGSDocument49 pagesCLINICAL PHARMACOLOGY OF CARDIOVASCULAR DRUGSfazry 415No ratings yet
- Clinical Pharmacology of Cardiovascular DiseasesDocument49 pagesClinical Pharmacology of Cardiovascular DiseaseservinasetianingsihNo ratings yet
- Lect 8 & 9 - Cardiovascular and NSAIDsDocument29 pagesLect 8 & 9 - Cardiovascular and NSAIDsRaneem ShiferNo ratings yet
- Penatalaksanaan Penyulit Gagal JantungDocument17 pagesPenatalaksanaan Penyulit Gagal JantungarumNo ratings yet
- Hipertensi EmergencyDocument31 pagesHipertensi Emergencyintan trimauliaNo ratings yet
- Cardiovascular System Achmad (Hypertension)Document27 pagesCardiovascular System Achmad (Hypertension)Hairul HasanNo ratings yet
- SPLE Clinical PharmaDocument72 pagesSPLE Clinical PharmaSEIYADU IBRAHIMNo ratings yet
- Cardiovascular-Renal DrugsDocument114 pagesCardiovascular-Renal DrugsShahpoor Ahmad ShirzadaNo ratings yet
- Crisis Hypertension: Dr. Isra Sukhraini NSTDocument21 pagesCrisis Hypertension: Dr. Isra Sukhraini NSTAndika SiswantaNo ratings yet
- Cardiogenic Shock and HemodynamicsDocument18 pagesCardiogenic Shock and HemodynamicsfikriNo ratings yet
- Blood Pressure Cardiac Output X Peripheral ResistanceDocument52 pagesBlood Pressure Cardiac Output X Peripheral Resistancelourdes kusumadiNo ratings yet
- P 3a Gagal JTGDocument35 pagesP 3a Gagal JTGAnaMariyaMaNo ratings yet
- HT Emergency Final DR Rinelia Minaswary, SPJPDocument46 pagesHT Emergency Final DR Rinelia Minaswary, SPJPAfdhal MuhammadNo ratings yet
- Diagnosis and Management of Shock: Dr. Nurkhalis, SPJP, FihaDocument49 pagesDiagnosis and Management of Shock: Dr. Nurkhalis, SPJP, FihaSiti rahmawatiNo ratings yet
- Congestive Cardiac Failure - Batch 8 Feb 2015Document79 pagesCongestive Cardiac Failure - Batch 8 Feb 2015frankozed1No ratings yet
- CardiomyopathyDocument17 pagesCardiomyopathysarguss1450% (2)
- AntihipertensiDocument39 pagesAntihipertensiHarri HardiNo ratings yet
- Cardiotonics - Dr Anoosha BhandarkarDocument60 pagesCardiotonics - Dr Anoosha BhandarkaranooshabhandarkarNo ratings yet
- Diagnosis and Management of Shock: Dr. Nurkhalis, SPJP, FihaDocument51 pagesDiagnosis and Management of Shock: Dr. Nurkhalis, SPJP, FihaHilmaNo ratings yet
- Hipertensi KrisisDocument30 pagesHipertensi KrisisLuthfan HakimNo ratings yet
- Atrial FibrillationDocument37 pagesAtrial Fibrillationapi-734449276No ratings yet
- Labetacure - Pregnancy HTN-1Document9 pagesLabetacure - Pregnancy HTN-1Omar Nassir MoftahNo ratings yet
- Terapi Cairan PD Syok KardiogenikDocument27 pagesTerapi Cairan PD Syok KardiogenikSri AsmawatiNo ratings yet
- 03 AntihypertensiveDocument89 pages03 Antihypertensive2nnfpjy5yvNo ratings yet
- Syok Kardiogenik Dr. Rani Maliawan, SP JPDocument59 pagesSyok Kardiogenik Dr. Rani Maliawan, SP JPLuh Leni AriniNo ratings yet
- Heart Failure & Cardiac Arrest: Rony YuliwansyahDocument92 pagesHeart Failure & Cardiac Arrest: Rony YuliwansyahSasha ManoNo ratings yet
- Cardiovasc Farmakologi Klinik0908Document49 pagesCardiovasc Farmakologi Klinik0908deka saputraNo ratings yet
- Antihypertensive Drugs: Dr. Dr. Nicolaski Lumbuun, SPFK Clinical Pharmacologist Faculty of MedicineDocument67 pagesAntihypertensive Drugs: Dr. Dr. Nicolaski Lumbuun, SPFK Clinical Pharmacologist Faculty of MedicineShally ChandraNo ratings yet
- Hipertensi PJK CHF STIKES WIKADocument62 pagesHipertensi PJK CHF STIKES WIKAKadek RiskiNo ratings yet
- Women Guideline FixDocument24 pagesWomen Guideline FixAndika SiswantaNo ratings yet
- Antihypertensive Drugs GuideDocument58 pagesAntihypertensive Drugs GuideadilaalifnugrahaeniNo ratings yet
- Hipertensi: DR, Suhaemi, SPPD, FinasimDocument110 pagesHipertensi: DR, Suhaemi, SPPD, FinasimNadya IndriatiNo ratings yet
- Congestive Heart Failure: Roy V, Jutzy, MDDocument46 pagesCongestive Heart Failure: Roy V, Jutzy, MDIrakiza jean jacquesNo ratings yet
- Cardiogenic ShockDocument41 pagesCardiogenic ShockOlga GoryachevaNo ratings yet
- Hipertensi PJK CHF (PSIK 2016)Document62 pagesHipertensi PJK CHF (PSIK 2016)Jasa Sunat JembranaNo ratings yet
- Cardiogenic Shock Hemodynamic ParametersDocument31 pagesCardiogenic Shock Hemodynamic ParameterscantikarevieraNo ratings yet
- What We Learn From The Newest Evidence ?Document70 pagesWhat We Learn From The Newest Evidence ?Intan HaddadNo ratings yet
- Plabable-Gems-19. Cardiology Plabable GemsDocument64 pagesPlabable-Gems-19. Cardiology Plabable GemsAli RazaNo ratings yet
- Hipertensi I, Dr. Dyah, SPJPDocument53 pagesHipertensi I, Dr. Dyah, SPJPSyerli MelintiNo ratings yet
- CCRN-PCCN-CMC Review Cardiac Part 2Document21 pagesCCRN-PCCN-CMC Review Cardiac Part 2Giovanni Mictil100% (1)
- Cardio Day 3: Hypertension, Hyperlipidemia, Arteriosclerosis, Ischemic Heart DiseaseDocument24 pagesCardio Day 3: Hypertension, Hyperlipidemia, Arteriosclerosis, Ischemic Heart DiseaseMikeNo ratings yet
- 1.1. Krisis Hipertensi - Dr. Saugi AbduhDocument29 pages1.1. Krisis Hipertensi - Dr. Saugi AbduhdmaulidaNo ratings yet
- Cardiogenic Shock and HemodynamicsDocument21 pagesCardiogenic Shock and Hemodynamicsravi_02No ratings yet
- Acute Heart Failure PDFDocument18 pagesAcute Heart Failure PDFRiaak ImNo ratings yet
- Congestive Heart Failure CHF: Dr. Suhaemi, SPPD, FinasimDocument94 pagesCongestive Heart Failure CHF: Dr. Suhaemi, SPPD, FinasimDella DevegaNo ratings yet
- Drugs Used in The Treatment of Congestive Heart FailureDocument18 pagesDrugs Used in The Treatment of Congestive Heart Failurekarina azlia amandaNo ratings yet
- Congestive Heart FailureDocument25 pagesCongestive Heart FailuredevianiamalinaNo ratings yet
- The Pathophysiology of Hypertension: Abdul Majid/ Eka Roina MDocument51 pagesThe Pathophysiology of Hypertension: Abdul Majid/ Eka Roina MYohanna SinuhajiNo ratings yet
- Internal Medicine: Over 200 Case StudiesFrom EverandInternal Medicine: Over 200 Case StudiesRating: 4.5 out of 5 stars4.5/5 (17)
- 1.1. Krisis Hipertensi - Dr. Saugi AbduhDocument29 pages1.1. Krisis Hipertensi - Dr. Saugi AbduhdmaulidaNo ratings yet
- Hypertensive Emergency 3Document45 pagesHypertensive Emergency 3saldy meirisandyNo ratings yet
- Hypertensive EmergenciesDocument28 pagesHypertensive EmergenciesluonganhsiNo ratings yet
- 4.krisis Hipertensi IMELS 15Document41 pages4.krisis Hipertensi IMELS 15putusanggraNo ratings yet
- Hipertensi PBLDocument41 pagesHipertensi PBLkholilgantengNo ratings yet
- Tatalaksana Krisis HipertensiDocument38 pagesTatalaksana Krisis HipertensiDr Edi HidayatNo ratings yet
- Cns PathologyDocument18 pagesCns Pathologysunnyorange8No ratings yet
- Hypertensive CrisisDocument30 pagesHypertensive CrisisAfraDewitaNo ratings yet
- Dr. Rahmah Safitri Meutia's Career History and Hypertension GuideDocument39 pagesDr. Rahmah Safitri Meutia's Career History and Hypertension GuidedhestiNo ratings yet
- Hypertensive Emergencies in The Emergency DepartmentDocument13 pagesHypertensive Emergencies in The Emergency DepartmentLuis Lopez RevelesNo ratings yet
- Chiranjeevi New Package List 2022Document109 pagesChiranjeevi New Package List 2022Shivam MittalNo ratings yet
- Hypertensive EmergenciesDocument49 pagesHypertensive EmergenciesSafa Abdualrahaman Ali HamadNo ratings yet
- Krisis Hipertensi IMELSDocument43 pagesKrisis Hipertensi IMELSrinadi_aNo ratings yet
- Crisis of Hypertension Revised 1Document57 pagesCrisis of Hypertension Revised 1keenmunir100% (4)
- Text Book Reading Hypertensive Encephalopathy: Fikri Fajrul FalahDocument16 pagesText Book Reading Hypertensive Encephalopathy: Fikri Fajrul FalahFikri Fajrul FalahNo ratings yet
- Krisis HipertensiDocument8 pagesKrisis HipertensiDr Edi HidayatNo ratings yet
- Krisis Hipertensi RevisiDocument44 pagesKrisis Hipertensi Revisidwi_bayu100% (1)
- Evaluation and Treatment of Hypertensive Emergencies in Adults - UpToDateDocument13 pagesEvaluation and Treatment of Hypertensive Emergencies in Adults - UpToDaterolland_arrizaNo ratings yet
- APSGNDocument3 pagesAPSGNmadimadi11No ratings yet
- Hipertensi PBLDocument41 pagesHipertensi PBLAl MuzakkiNo ratings yet
- Management of Hypertensive Elderly in Clinical Dentistry: Patcharaphol Samnieng, Kantapong PloydanaiDocument9 pagesManagement of Hypertensive Elderly in Clinical Dentistry: Patcharaphol Samnieng, Kantapong PloydanaiSatya AsatyaNo ratings yet
- GREY BOOK August 2020 71st EditionDocument156 pagesGREY BOOK August 2020 71st EditionChris Jardine LiNo ratings yet
- Hypertensive EncephalopathyDocument7 pagesHypertensive Encephalopathymery indrawatiNo ratings yet
- Management of Hypertensive Crisis: British and Irish Hypertension Society Position DocumentDocument17 pagesManagement of Hypertensive Crisis: British and Irish Hypertension Society Position DocumentPaula SantosNo ratings yet
- Hypertensive Emergency, El - ShahawyDocument41 pagesHypertensive Emergency, El - ShahawysalwaNo ratings yet
- Hypertensive Emergencies (ESC 2019)Document10 pagesHypertensive Emergencies (ESC 2019)Glen LazarusNo ratings yet
- A Literature Review On Hypertensive Crisis: European Journal of Pharmaceutical and Medical ResearchDocument6 pagesA Literature Review On Hypertensive Crisis: European Journal of Pharmaceutical and Medical ResearchCindy MaslagNo ratings yet
- Providing Prompt Medical Care for Major EmergenciesDocument78 pagesProviding Prompt Medical Care for Major EmergenciesGopala Hari100% (8)
- Erythropoietin 2Document12 pagesErythropoietin 2jolie_victoriaNo ratings yet