You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- PSR 11 917 MDocument2 pagesPSR 11 917 Mpeterson_msc5No ratings yet
- Daikin Altherma 3 R - ERLA-D Series - Product Catalogue - ECPEN22-738 - EnglishDocument44 pagesDaikin Altherma 3 R - ERLA-D Series - Product Catalogue - ECPEN22-738 - Englishervin.hvaclabNo ratings yet
- CVS ExaminationDocument72 pagesCVS ExaminationPrashanthBhatNo ratings yet
- I. Demographic Profile: Treatments/MedicationDocument4 pagesI. Demographic Profile: Treatments/MedicationGrace MellaineNo ratings yet
- Press Release: Semarang, 22 October 2017 - PT Kalbe Farma TBK (Kalbe) Through Kalbe EthicalDocument2 pagesPress Release: Semarang, 22 October 2017 - PT Kalbe Farma TBK (Kalbe) Through Kalbe EthicalYessy YasmaraldaNo ratings yet
- All CodesDocument279 pagesAll CodesiceyrosesNo ratings yet
- Daily Checklist: YES YES YES YES YES X YESDocument47 pagesDaily Checklist: YES YES YES YES YES X YESEdmar TabinasNo ratings yet
- CXG - 069e Guideline For The Validation of Food Safety Control MeasuresDocument10 pagesCXG - 069e Guideline For The Validation of Food Safety Control MeasuresYêu Thời Trang SophieParisNo ratings yet
- Pro-Choice Violence in ArkansasDocument6 pagesPro-Choice Violence in ArkansasHuman Life InternationalNo ratings yet
- Visual ImpairmentDocument7 pagesVisual ImpairmentROSE MARIE REVILLA100% (1)
- HU038 - Humes Oasis 2000 Series Owners Manual v6 WEBDocument22 pagesHU038 - Humes Oasis 2000 Series Owners Manual v6 WEBCodrut DavidNo ratings yet
- Classification of Engines & Its ComponentsDocument33 pagesClassification of Engines & Its ComponentsSunil DhankharNo ratings yet
- Comparing and Cross Matching (1.3) EIM NC IIDocument2 pagesComparing and Cross Matching (1.3) EIM NC IIHarvey RamosNo ratings yet
- Tarnished Queen - Nicole FoxDocument396 pagesTarnished Queen - Nicole Foxyourmom33% (3)
- TL280LE (R) : Internet and LTE/HSPA Dual-Path Alarm CommunicatorDocument60 pagesTL280LE (R) : Internet and LTE/HSPA Dual-Path Alarm Communicatorcchung147554No ratings yet
- Spinal Cord Anatomy and Localization.4Document18 pagesSpinal Cord Anatomy and Localization.4Dalwadi1No ratings yet
- MAN Marine Auxiliary Engines 2018 1Document1 pageMAN Marine Auxiliary Engines 2018 1Tudor AgheorghieseiNo ratings yet
- 2018 QMS Asphalt ManualDocument364 pages2018 QMS Asphalt ManualhabtamualemNo ratings yet
- AC Rectifier Bulk Capacitor Selection With Analysis+SPICE (Walker) PDFDocument5 pagesAC Rectifier Bulk Capacitor Selection With Analysis+SPICE (Walker) PDFjazbo8No ratings yet
- Early Adolescent Lumbar Intervertebral Disc Injury: A Case StudyDocument7 pagesEarly Adolescent Lumbar Intervertebral Disc Injury: A Case StudyfeliNo ratings yet
- Book PHARMACEUTICS 1Document85 pagesBook PHARMACEUTICS 1Muhammad sajjad93% (14)
- LGDocument9 pagesLGSandeep SinglaNo ratings yet
- Casa de Moda DolcegabbanaDocument4 pagesCasa de Moda Dolcegabbanadianaionelav23No ratings yet
- Clinical Hyperbaric Facility Accreditation Manual 2005 Edition (Revision 1)Document83 pagesClinical Hyperbaric Facility Accreditation Manual 2005 Edition (Revision 1)Paulo Costa SilvaNo ratings yet
- Duties and Qualities of A ButlerDocument6 pagesDuties and Qualities of A ButlerZiquerzMarkuz100% (1)
- Hydraulic Accumulator - Test and Charge: Cerrar SIS Pantalla AnteriorDocument9 pagesHydraulic Accumulator - Test and Charge: Cerrar SIS Pantalla AnteriorHomer Yoel Nieto Mendoza100% (1)
- Seismic InterpretationDocument23 pagesSeismic Interpretationnasir.hdip8468No ratings yet
- Huda Munir McqsDocument21 pagesHuda Munir McqsAngelo P. VeluzNo ratings yet
- MODULE in Stat Week 6Document10 pagesMODULE in Stat Week 6Joshua GonzalesNo ratings yet
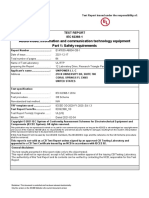
- Audio/video, Information and Communication Technology Equipment Part 1: Safety RequirementsDocument168 pagesAudio/video, Information and Communication Technology Equipment Part 1: Safety RequirementsneodvxNo ratings yet