METACARPAL FRACTURES
Jinnasit Hongtrakul
22/12/60
�• Hand fractures can be complicated by deformity from no treatment,
stiffness from overtreatment and both deformity and stiffness from
poor treatment.
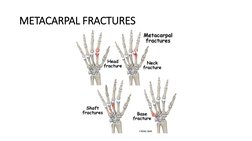
�METACARPAL FRACTURES
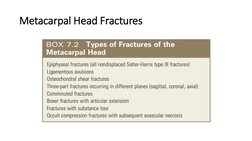
�Metacarpal Head Fractures
�Metacarpal Head Fractures
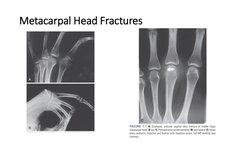
• Comminuted fractures occurred most commonly.
• Index most frequently
• Mechanism: axial load or direct trauma
• X-ray: PA, lat , oblique and brewerton view
• Articular defects may remodel with time, MP joint may function
satisfactorily with painless motion.
• Treatment of these fractures must be individualized.
�Metacarpal Head Fractures
• Displaced ligament avulsion fractures
• Osteochondral fractures
can be satisfactorily managed by ORIF
• If 2 part Kirschner wires or interfragmentary screws.
• Comminuted articular fracture
• Bone loss
• ORIF may be frustrating
• Skeletal traction or joint arthroplasty
�Metacarpal Head Fractures
• Displaced fractures that constitute more than 25% of the articular
surface or exhibit more than 1mm of articular step-off are treated
operatively
• Two-part articular fractures are usually amenable to fixation with
headless screws. Fixation with Kirschner wires, although easier, is
less rigid and requires immobilization for 3 to 4 weeks. with the
MP joint flexed 70 degrees,
• Unstable reductions may require immobilization for 2 to 3
weeks before range-of-motion exercises are begun
�Metacarpal Head Fractures
�Metacarpal Head Fractures
• Skeletal traction or external fixation may be needed if there are
associated comminuted fractures of the adjacent base
of the proximal phalanx.
• Arthroplasty is a reasonable alternative
Should not be done
• [Link] of the head of the index finger because shear stresses from
pinch predictably result in implant failure
2. Inadequate soft tissue coverage
3. Excessive metacarpal bone loss because excessive shortening and
instability occur
�Metacarpal Neck Fractures
• Common in ring and little finger
• Character: Apex dorsal angulation
• comminution of the volar metacarpal neck
• Intrinsic muscles that cross the MP joint lie volar to its axis of rotation
• mechanism: clenched MCP strikes a solid object
�Metacarpal Neck Fractures
• Malrotation is the main problems
• prominence of the metacarpal head,
• Diminished range of motion,
• Palpable metacarpal head in the palm
• factors must be considered:
• (1) which metacarpal neck is fractured.
• (2) the degree of angulation
• (3) presence of a rotational deformity.
• (4) Pseudoclawing finger : excessive metacarpal neck, MP hyperextension, PIP
flexion
�Metacarpal Neck Fractures
• Closed Reduction of Metacarpal Neck Fractures
• Jahss’s maneuver: 90 MCP flexion (relax intrinsic muscle, tightening collateral
ligament)
: 90 PIP flexion
: Upward pressure through the proximal phalanx
: Downward pressure on the metacarpal shaft
Immobilization : Gutter cast , Clam-digger cast 3-6 weeks
• Closed reduction and percutaneous pinning
• Open Reduction of Metacarpal Neck Fractures
• Manipulation fails to restore acceptable angulatory or rotational alignment.
• Used wires or tension band or miniplate fixation.
�Metacarpal Neck Fractures
• Indication for implant fixation
• Reduction is unacceptable or cannot be maintained
10-15 degrees in the index and middle fingers
30-40 degrees in the ring finger
50-60 degrees in the little finger
�Metacarpal Neck Fractures
�Metacarpal Neck Fractures
• Implants fixation
• Closed percutaneous cross/longitudinal K-wires fixation
• Closed transmetacarpal K-wire fixation
• Closed percutaneous intramedullary K-wires fixation “Bouquet”
• ORIF with tension band wire loop
• ORIF with miniplate and screws
�Metacarpal Neck Fractures
�Metacarpal Neck Fractures
�Metacarpal
Neck
Fractures
�Metacarpal Shaft Fractures
Classified into three types : Transverse, Oblique (spiral), Comminuted
• Transverse fractures
• Mechanism : Axial loading, direct blow
• Interosseous muscle : deforming force ; Apex dorsal
• Acceptable angulation
• Index and Middle finger : 10-20 degrees
• Ring finger : 20-30 degrees
• Little finger : 30-40 degrees
• Shortening 2-5 mm
�Metacarpal Shaft Fractures
• Dorsal angulation has several undesirable effects
• 1. The metacarpal head becomes prominent in the palm and may cause pain
on grasping.
• 2. There may be compensatory hyperextension at the MP joint that results in
a secondary pseudoclaw deformity with digital extension.
• 3. Patients find the dorsal prominence aesthetically displeasing.
• 4. There is metacarpal shortening; if great enough, the intrinsic muscles
may be unable to accommodate and are consequently weakened
�Metacarpal Shaft Fractures
• Oblique fractures
• Mechanism: torsional forces
• Can cause rotational malalignment.
• patient flex all the fingers simultaneously If scissoring or malrotation is
present with composite digital flexion open reduction should be
considered.
• Comminuted fractures
• Mechanism: direct impact , often associated with soft tissue injury
• associated with soft tissue injury, and may produce shortening.
�Metacarpal Shaft Fractures
• Treatment
• Most can be treated nonoperatively.
• Nondisplaced, stable fracture : Clam-digger cast 4 weeks
Clam-digger cast : Short-arm cast with dorsal extension block of MP joint.
Position : Wrist in 30-40 degrees of extension
: MP in 80-90 degrees of flexion
: IP in full extension
: Intrinsic-plus (clam-digger) position
: Limits joints contracture and relax intrinsic muscle force
�Metacarpal Shaft Fractures
�Metacarpal Shaft Fractures
• Closed reduction and percutaneous pinning
• Indication: when fractures can closed reduce but unable to maintain in cast
• ORIF Indication:
1. Open fractures
2. Multiple fractures that stabilizing effect of the adjacent metacarpal is lost
3. Unstable fracture that cannot be held by closed percutaneous
4. Malaligment Malrotation
�Metacarpal
Shaft
Fractures
�Metacarpal Shaft Fractures
�Metacarpal Shaft Fractures
�Metacarpal
Shaft Fractures
�Metacarpal Shaft Fractures
�Segmental Metacarpal Loss
• Restoration of hand function is usually staged and begins with
thorough débridement of devitalized tissue.
• maintaining metacarpal length with transverse intermetacarpal
Kirschner wires or external fxation devices
• Bone grafting is performed only after joint motion is regained and
healed wounds have matured.
• The best time to restore osseous stability with a bone graft and
internal fixation is within the first 10 days of injury
�Segmental Metacarpal Loss
• Reconstitution of osseous stability involves two steps:
1. Provisional stabilization
Maintenance of metacarpal length
transfixation pins
external fixation
methyl methacrylate spacers
combinations of these techniques.
2. Bone grafting with or without internal fixation
Most defects can be bridged with autogenous iliac corticocancellous graft.
�Segmental Metacarpal Loss
�Segmental Metacarpal Loss
�Metacarpal Base Fractures and Carpometacarpal
Fracture-Dislocations
• Avulsion Factures of the Second and Third Metacarpal Bases
- Rare
- Usually result of a fall on a palmar flexed wrist
• Isolated ring finger metacarpal fractures should raise the possibility
of an associated CMC joint injury
• Fracture dislocations of the small finger CMC joint
• Intra-articular fracture of the Hamate-fifth metacarpal joint are common
• Associated with proximal and dorsal subluxation of the metacarpal.
• Similar to Bennett’s fracture
�Metacarpal Base Fractures and Carpometacarpal
Fracture-Dislocations
• Pull of ECU and FCU through Pisometacarpal ligament : displacement
and proximal migration
• Pull of Abductor digiti minimi and slope of hamate : 5th CMC joint
instability
• Radiography : plain x-ray : is often missed
• Special view
• -Bora and Didizian : AP view with forearm pronated 30 degrees from fully
supinated position
�Metacarpal Base Fractures and Carpometacarpal
Fracture-Dislocations
• Closed reduction and percutaneous pinning ; prefer
• ORIF with metacarpal pin : optional
• Surgical treatment was not strong because arthrodesis of the joint
could always be performed for persistent pain.
• Restoration of the articular surface should be the goal of treatment.
• comminuted dorsal hamate fractures or coronal shear fractures
through the hamate, were particularly unstable, and ORIF was
uniformly necessary.
�Metacarpal Base Fractures and Carpometacarpal
Fracture-Dislocations
�Metacarpal Base Fractures and Carpometacarpal
Fracture-Dislocations
• If a fracture-dislocation of the fifth CMC joint is seen more than 3
weeks after the injury, we prefer to accept the alignment.
If symptomatic arthritis develops, secondary arthrodesis can be
performed.
�Multiple Carpometacarpal Dislocations
• Multiple CMC dislocations are high-energy injuries that nearly
always require ORIF.
• reduction with Kirschner pin fixation was recommended.
�Complications of Metacarpal Fractures
• Malunion
• Angulation
: Most are dorsal angulation
: Result of transverse shaft fracture
: Painful and weak grip
: 2nd, 3rd angulation : particularly bothersome both cosmetically and
functionally
: Treatment Closing wedge osteotomy ,Opening wedge if metacarpal is
shortened
• Rotation
: Result from spiral or oblique fracture
: Overlapping of fingers ( scissoring )
: Treatment Corrective osteotomy though base of metacarpal.
�Complications of Metacarpal Fractures
• Malunion
• Intraarticular
: Rarely amendable to corrective osteotomy
: If fracture line is visualized and bone stock is adequate, corrective osteotomy
�Complications of Metacarpal Fractures
�Complications of Metacarpal Fractures
�Complications of Metacarpal Fractures
• Osteomyelitis : Rare
: High amputation rate: if delayed in treatment > 6 months or >3 operations required
: Treatment - Adequate debridement
- Systemic antibiotic at least 4-6 weeks
- External fixation
- Antibiotic-impregnated cement can be supplemented
- If infection is cleared, Bone grafting and internal fixation will be done
• Nonunion : Most are atropic or hypovascular
: Treatment - Resection pseudarthrosis
- Bone graft
- Stable internal fixation
�THANK YOU