You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Sample Test Questions For The CPC ExamDocument8 pagesSample Test Questions For The CPC ExamHarikaSabbineni100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Physical Therapy DocumentationDocument5 pagesPhysical Therapy DocumentationdjdkNo ratings yet
- Gastroenterol. Rep. Gastro - Got015, Figure 1Document1 pageGastroenterol. Rep. Gastro - Got015, Figure 1Decky Aditya ZNo ratings yet
- Drug Food InteractionsDocument8 pagesDrug Food InteractionsDecky Aditya ZNo ratings yet
- Plasmid Recombinant Technique: E. Coli and Carrying Two Gene: AmpDocument6 pagesPlasmid Recombinant Technique: E. Coli and Carrying Two Gene: AmpDecky Aditya ZNo ratings yet
- Laporan Tutorial Skenario V: Genetic Engineering: TUTOR: Dr. Nurhidayati, M. KesDocument37 pagesLaporan Tutorial Skenario V: Genetic Engineering: TUTOR: Dr. Nurhidayati, M. KesDecky Aditya ZNo ratings yet
- Full Mouth RehabDocument9 pagesFull Mouth RehabpragatiNo ratings yet
- Obtundents, Mummifying Agents and FluoridesDocument11 pagesObtundents, Mummifying Agents and Fluoridesrupesh dalaviNo ratings yet
- Format Baru Reten Hiv 2015 (MCH Punya)Document3 pagesFormat Baru Reten Hiv 2015 (MCH Punya)Hazim RosliNo ratings yet
- Ue Gen PathologyDocument287 pagesUe Gen PathologyReza RastgooNo ratings yet
- Nursing Notes 4Document3 pagesNursing Notes 4karan SinghNo ratings yet
- Mnemonic SDocument10 pagesMnemonic SAli HabibNo ratings yet
- Helicobacter Pylori: Brianán Mcgovern (Microbiology SPR)Document35 pagesHelicobacter Pylori: Brianán Mcgovern (Microbiology SPR)Omkar PotnisNo ratings yet
- Failure To ThriveDocument11 pagesFailure To ThriveAngky Rofi IrwansyahNo ratings yet
- 1 5041847269662392377 PDFDocument378 pages1 5041847269662392377 PDFMauro DucattiNo ratings yet
- ASSESSMENTDocument2 pagesASSESSMENTCuttie Anne GalangNo ratings yet
- Fluids and ElectrolytesDocument31 pagesFluids and ElectrolytesUmarNo ratings yet
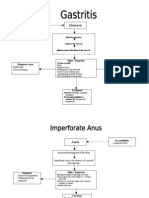
- Gastro PathophysiologyDocument4 pagesGastro PathophysiologyPaul JoloNo ratings yet
- Handout 10 Circulatory SystemDocument2 pagesHandout 10 Circulatory SystemKyle QuietaNo ratings yet
- Proposed Decision by Judge Teri L. BlockDocument33 pagesProposed Decision by Judge Teri L. Blockjon_ortizNo ratings yet
- Extricare-2400 IFU PDFDocument24 pagesExtricare-2400 IFU PDFShankar Madhukarrao BahureNo ratings yet
- Cebu CFI Coop Annual Report 2013Document2 pagesCebu CFI Coop Annual Report 2013Mark C. Herrera100% (1)
- Minimum Inhibitory Concenration (Mic)Document13 pagesMinimum Inhibitory Concenration (Mic)iinNo ratings yet
- Implant Connections Website enDocument13 pagesImplant Connections Website enCatalin PopescuNo ratings yet
- Mindanao State University - Iligan Institute of Technology College of NursingDocument5 pagesMindanao State University - Iligan Institute of Technology College of NursingNessy Nicholle SatruionNo ratings yet
- Observation Sheet For Body Aesthetic TreatmentDocument3 pagesObservation Sheet For Body Aesthetic TreatmentScribdTranslationsNo ratings yet
- CimetidineDocument3 pagesCimetidineapi-3797941No ratings yet
- Brochure DVE Laser Film 201505Document2 pagesBrochure DVE Laser Film 201505RDII YANMEDRSDSNo ratings yet
- Herniated Lumbar Intervertebral DiskDocument10 pagesHerniated Lumbar Intervertebral DiskRoberto López MataNo ratings yet
- Assessment A Critically Ill PatientDocument23 pagesAssessment A Critically Ill PatientJorelyn Frias100% (1)
- Diagnostic Medical SonographyDocument14 pagesDiagnostic Medical SonographyJeyarajasekar TtrNo ratings yet
- Pharmacy Cbahi Questions 2022Document12 pagesPharmacy Cbahi Questions 2022osama hosni100% (1)
- Accenture - Artificial Intelligence - Healthcare's New Nervous SystemDocument8 pagesAccenture - Artificial Intelligence - Healthcare's New Nervous SystemRobert KoverNo ratings yet
- Fire Technician CV - Abdullah AlhajriDocument2 pagesFire Technician CV - Abdullah AlhajriMohammed Saeed100% (1)