You might also like
- Report On Induced Abortion - Methods of Termination of Pregnancy Till 12 Wks of Gestation, Pre Abortion CounselingDocument4 pagesReport On Induced Abortion - Methods of Termination of Pregnancy Till 12 Wks of Gestation, Pre Abortion CounselingAdnan Akram, MD (Latvia)No ratings yet
- Tmbool's Notes in Obstetrics and Gynecology PDFDocument113 pagesTmbool's Notes in Obstetrics and Gynecology PDFOsman SomiNo ratings yet
- Worth A ShotDocument9 pagesWorth A ShotAngie VelascoNo ratings yet
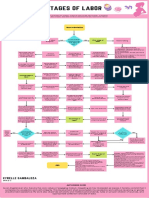
- Stages of Labor FlowchartDocument1 pageStages of Labor FlowchartXyrelle GambalozaNo ratings yet
- Fetoplacental DeficiencyDocument16 pagesFetoplacental DeficiencyОлександра ЗагородняNo ratings yet
- Early Pregnancy Bleeding: 1. Abortion 2. Ectopic Pregnancy 3. GTDDocument48 pagesEarly Pregnancy Bleeding: 1. Abortion 2. Ectopic Pregnancy 3. GTDGebremichael Reta100% (2)
- Preterm LaborDocument4 pagesPreterm Labormruts aregawiNo ratings yet
- CME PRETERM LABOR, PROM, PPROM FDocument39 pagesCME PRETERM LABOR, PROM, PPROM FRatna Setia WatiNo ratings yet
- Case 2 TG Retype PDFDocument15 pagesCase 2 TG Retype PDFElma CorpusNo ratings yet
- 2.early Pregnancy and BleedingDocument79 pages2.early Pregnancy and BleedingjosephNo ratings yet
- IT 5 - Kehamilan Preterm Postterm - FTHDocument31 pagesIT 5 - Kehamilan Preterm Postterm - FTHShidqiNo ratings yet
- Handouts Ob AbnormalDocument16 pagesHandouts Ob AbnormalShenn ChavezNo ratings yet
- EC PregDocument58 pagesEC PregCaryl Kay CallangaNo ratings yet
- Preterm Labour: Management GuidelinesDocument44 pagesPreterm Labour: Management Guidelinesvacha sardarNo ratings yet
- Preterm Labour: Muhammad Hanif Final Year MBBSDocument32 pagesPreterm Labour: Muhammad Hanif Final Year MBBSArslan HassanNo ratings yet
- Preterm Postterm Prom1Document35 pagesPreterm Postterm Prom1api-3856051No ratings yet
- Pre and Post PregnancyDocument23 pagesPre and Post PregnancyJitendra ChaudharyNo ratings yet
- Ptl/Pprom and Multifetal Gestation: Anna Buabbud MD Ms3 LectureDocument38 pagesPtl/Pprom and Multifetal Gestation: Anna Buabbud MD Ms3 LectureNik C0% (1)
- Placenta Previa 08Document42 pagesPlacenta Previa 08Sam Ngugi100% (1)
- 3-Management of Abortion and Postabortion CareDocument22 pages3-Management of Abortion and Postabortion CareBekeNo ratings yet
- 12 Antepartum HemorrhageDocument10 pages12 Antepartum HemorrhageJuan RamirezNo ratings yet
- BLEEDING IN EARLY PREGNANCYDocument36 pagesBLEEDING IN EARLY PREGNANCYvictor onapaNo ratings yet
- Ch. 21+22Document11 pagesCh. 21+22Gailstar GutierrezNo ratings yet
- Pregnancy Complication Differentials and ExplainDocument9 pagesPregnancy Complication Differentials and ExplainJeffrey XieNo ratings yet
- Early Pregnancy Complications (Abortion & Ectopic Pregnancy)Document61 pagesEarly Pregnancy Complications (Abortion & Ectopic Pregnancy)በአምላክ ጋሻዬ በዛNo ratings yet
- Preterm Labor-1Document28 pagesPreterm Labor-1tajfaiz779No ratings yet
- Preterm Labour and Birth (Latest)Document43 pagesPreterm Labour and Birth (Latest)Nur Aliah Amirah AmranNo ratings yet
- Dr. Deviana S. Riu, SpogDocument19 pagesDr. Deviana S. Riu, SpogmasyfuqNo ratings yet
- Dysfunction of The Genito-Urinary Tract: Dejene Edosa (BSC, MSC in CMW) July 2021Document25 pagesDysfunction of The Genito-Urinary Tract: Dejene Edosa (BSC, MSC in CMW) July 2021michaelNo ratings yet
- Premature Rupture of MembranesDocument29 pagesPremature Rupture of MembranesIda YosopaNo ratings yet
- Contraception and AbortionDocument20 pagesContraception and Abortiondaniel mitikuNo ratings yet
- Miscarriage Preterm Labor: Obstetrics and Gynecology Lyzikova Yu.ADocument36 pagesMiscarriage Preterm Labor: Obstetrics and Gynecology Lyzikova Yu.AMed PoxNo ratings yet
- Antepartum Care: Preconception and Prenatal CareDocument60 pagesAntepartum Care: Preconception and Prenatal CareAbdul Rahman NarawiNo ratings yet
- Preterm LaborDocument33 pagesPreterm LaborChristian MolinaNo ratings yet
- Preventing Preterm Birth: Risk Factors, Signs, and ManagementDocument24 pagesPreventing Preterm Birth: Risk Factors, Signs, and ManagementNidya PutriNo ratings yet
- Induction and AugmentationDocument44 pagesInduction and AugmentationzulinassirNo ratings yet
- Ob Management Septic AbortionDocument8 pagesOb Management Septic AbortionspringdingNo ratings yet
- ECTOPIC PREGNANCY - OB PATHODocument32 pagesECTOPIC PREGNANCY - OB PATHONorman Vryne CaduaNo ratings yet
- Guide to Induction of Labour Methods and TechniquesDocument5 pagesGuide to Induction of Labour Methods and TechniquesSuhashis MukherjeeNo ratings yet
- Early Pregnancy Bleeding Diagnosis and ManagementDocument79 pagesEarly Pregnancy Bleeding Diagnosis and ManagementFeroz Haniff AzmaiNo ratings yet
- Abortion: By: Priyanka Sadafule 1 Year PBBSC Student SeminarDocument51 pagesAbortion: By: Priyanka Sadafule 1 Year PBBSC Student SeminarDigu SadafuleNo ratings yet
- Bleeding in Early PregnancyDocument4 pagesBleeding in Early Pregnancynur1146No ratings yet
- Clinical Findings: ACOG - Cervical Insufficiency As "Document5 pagesClinical Findings: ACOG - Cervical Insufficiency As "lllNo ratings yet
- Spontaneous MiscarriageDocument14 pagesSpontaneous MiscarriageGomez VanessaNo ratings yet
- Infections of The Upper Genital TractDocument40 pagesInfections of The Upper Genital TractBernard Palarca SantosNo ratings yet
- Maternal Child Nursing ModuleDocument7 pagesMaternal Child Nursing ModuleWizzardNo ratings yet
- Early Pregnancy CME Hyrax 2.10Document31 pagesEarly Pregnancy CME Hyrax 2.10Alice KaariaNo ratings yet
- AbortionDocument30 pagesAbortionKIYANo ratings yet
- Preterm LaborDocument62 pagesPreterm LaborAstri Sri Widiastuty100% (1)
- "Prevention of Preterm Parturition": Journal ReadingDocument23 pages"Prevention of Preterm Parturition": Journal ReadingRettyNo ratings yet
- Etopic PregnancyDocument15 pagesEtopic PregnancyAileenNo ratings yet
- طوارئ توليدية 5,6&7Document10 pagesطوارئ توليدية 5,6&7HamzahNo ratings yet
- POST TERM PREGNANCY RISKSDocument14 pagesPOST TERM PREGNANCY RISKSPaul Behring ManurungNo ratings yet
- Antepartum HemorrhageDocument22 pagesAntepartum HemorrhageGetaneh LiknawNo ratings yet
- Tocolytics (Also Called Anti-Contraction Medications or Labor Represents) AreDocument2 pagesTocolytics (Also Called Anti-Contraction Medications or Labor Represents) AreEric RothNo ratings yet
- Miscarriage (Abortion) : (Adhesions Inside The Uterine Cavity)Document10 pagesMiscarriage (Abortion) : (Adhesions Inside The Uterine Cavity)Rashed Shatnawi100% (1)
- Balang Basta Way PasalubongDocument16 pagesBalang Basta Way Pasalubongjovan teopizNo ratings yet
- AbortionDocument67 pagesAbortionaneley cherinetNo ratings yet
- Spontaneous Abortion (Miscarriage) Definition:: SyndromeDocument9 pagesSpontaneous Abortion (Miscarriage) Definition:: SyndromeSridevi DevarajNo ratings yet
- Emergency Obstetrics1Document74 pagesEmergency Obstetrics1Alphine DalgoNo ratings yet
- Pre-Menopause, Menopause and Beyond: Volume 5: Frontiers in Gynecological EndocrinologyFrom EverandPre-Menopause, Menopause and Beyond: Volume 5: Frontiers in Gynecological EndocrinologyMartin BirkhaeuserNo ratings yet
- Preterm Labor 2Document18 pagesPreterm Labor 2Олександра ЗагородняNo ratings yet
- Preterm LaborDocument19 pagesPreterm LaborОлександра ЗагородняNo ratings yet
- Lecture 1physiology of PregnancyDocument15 pagesLecture 1physiology of PregnancyОлександра ЗагородняNo ratings yet
- Lecture 1physiology of PregnancyDocument58 pagesLecture 1physiology of PregnancyОлександра ЗагородняNo ratings yet
- Jurnal Plasenta Akreta PDFDocument5 pagesJurnal Plasenta Akreta PDFfatqur28No ratings yet
- Gillick Fraser guidelinesDocument1 pageGillick Fraser guidelinesStacyNo ratings yet
- Estimation of Degree of CalcinationDocument30 pagesEstimation of Degree of CalcinationRashmi100% (1)
- 18 Month QuestionnaireDocument6 pages18 Month QuestionnaireAnnie AbreuNo ratings yet
- Health Talk On ContraceptionDocument17 pagesHealth Talk On ContraceptionSandhya sNo ratings yet
- Sleep Handout: Dr. Todd WolynnDocument17 pagesSleep Handout: Dr. Todd WolynnSimona MariaNo ratings yet
- "My Parents Are Gay": Lived Experiences of Children With Lesbian ParentsDocument59 pages"My Parents Are Gay": Lived Experiences of Children With Lesbian ParentsAlyssa LopezNo ratings yet
- Chapter24 PDFDocument43 pagesChapter24 PDFCindy MaslagNo ratings yet
- Families Around The WorldDocument3 pagesFamilies Around The WorldYurlay PajaroNo ratings yet
- Preventive Paediatric and Paediatric NursingDocument2 pagesPreventive Paediatric and Paediatric NursingHUSSAINA BANONo ratings yet
- Veterinary Gynaecology ObstetricsDocument8 pagesVeterinary Gynaecology ObstetricsSuryakantaRoulTuntunNo ratings yet
- Weiss Functional Impa Irment Rating Scale - Parent REPORt (WFIRS-P)Document2 pagesWeiss Functional Impa Irment Rating Scale - Parent REPORt (WFIRS-P)Subhan AnsariNo ratings yet
- Let Them Eat DirtDocument2 pagesLet Them Eat DirtSouthern California Public Radio0% (1)
- Amazing Things Happen When Student Nurses Are Given Birth Doula TrainingDocument7 pagesAmazing Things Happen When Student Nurses Are Given Birth Doula TrainingDeni FitriNo ratings yet
- Dr. Lilia JamisseDocument1 pageDr. Lilia JamisseNewborn2013No ratings yet
- Chapter 15 - Moral Development and AggressionDocument31 pagesChapter 15 - Moral Development and Aggressionlalonde.devonNo ratings yet
- Birthweight and Survival in Lambs, Oldham Et Al, 2011Document8 pagesBirthweight and Survival in Lambs, Oldham Et Al, 2011Jesús Enrique Turín VilcaNo ratings yet
- Amniocentesis: Contact: Innoclazz Academy For Best Home Tutors in Bangalore, Hyderabad, Chennai, Mumbai and Pune WebsiteDocument14 pagesAmniocentesis: Contact: Innoclazz Academy For Best Home Tutors in Bangalore, Hyderabad, Chennai, Mumbai and Pune WebsiteInnoclazz AcademyNo ratings yet
- Policy Responses Low Fertility UNFPA WP Final Corrections 7feb2020 CLEANDocument98 pagesPolicy Responses Low Fertility UNFPA WP Final Corrections 7feb2020 CLEANNatalia GuinsburgNo ratings yet
- Advancing Healthy Births Plan 2024 To 2028Document30 pagesAdvancing Healthy Births Plan 2024 To 2028WXMINo ratings yet
- PPH Case StudyDocument76 pagesPPH Case StudyDhanashree Anil Pore100% (31)
- Ideas For Using Books To Support Social Emotional DevelopmentDocument8 pagesIdeas For Using Books To Support Social Emotional DevelopmentNikoletta KouskouniNo ratings yet
- Pedia 1Document4 pagesPedia 1Aijem Ryan100% (2)
- Book NameDocument8 pagesBook NameSAGAR ADHAONo ratings yet
- Low Rates of Pregnancy Termination For Prenatally Diagnosed Klinefelter Syndrome and Other Sex Chromosome PolysomiesDocument5 pagesLow Rates of Pregnancy Termination For Prenatally Diagnosed Klinefelter Syndrome and Other Sex Chromosome PolysomiesAltaicaNo ratings yet
- Original PDF Parent Child Relations An Introduction To Parenting 10th Edition PDFDocument41 pagesOriginal PDF Parent Child Relations An Introduction To Parenting 10th Edition PDFkatharine.boyd469100% (29)
- Cultural Child Rearing Practices in ToddlerhoodDocument11 pagesCultural Child Rearing Practices in Toddlerhoodapi-604124393No ratings yet
- Psychological Theories and ModelsDocument13 pagesPsychological Theories and ModelsLuluk QurrotaNo ratings yet