You might also like
- What Is Orgone EnergyDocument19 pagesWhat Is Orgone EnergyRadu Badoiu100% (2)
- Ayurvedic Detoxification: How To Cleanse SafelyDocument14 pagesAyurvedic Detoxification: How To Cleanse Safelydynamic2004No ratings yet
- Yearning of The SoulDocument97 pagesYearning of The SoulViraj PanaraNo ratings yet
- (Ebook) FSVP - A Comprehensive GuideDocument16 pages(Ebook) FSVP - A Comprehensive Guidesajid waqasNo ratings yet
- Increases in COVID 19 Are Unrelated To Levels of Vaccination Across 68 Countries and 2947 Counties in The United StatesDocument4 pagesIncreases in COVID 19 Are Unrelated To Levels of Vaccination Across 68 Countries and 2947 Counties in The United StatesKyle Becker95% (19)
- OR 01a FCDocument12 pagesOR 01a FCfritzrose50% (2)
- Hydrocortisone PDFDocument4 pagesHydrocortisone PDFsangita bssmetNo ratings yet
- DR Sudhir Bhandari Final Presentation 12-4-2021 NewDocument67 pagesDR Sudhir Bhandari Final Presentation 12-4-2021 NewsurruNo ratings yet
- Diagnostik Dasar Radiologis COVID-19Document42 pagesDiagnostik Dasar Radiologis COVID-19tenty isniNo ratings yet
- Miliary Tuberculosis With Severe Pneumonia Without Abnormal Chest Sounds in A Covid 19 PandemicDocument4 pagesMiliary Tuberculosis With Severe Pneumonia Without Abnormal Chest Sounds in A Covid 19 PandemicMelly SyafridaNo ratings yet
- 1 s2.0 S2590041221000039 MainDocument2 pages1 s2.0 S2590041221000039 MainMa No LoNo ratings yet
- COVID 19 RadiologyDocument29 pagesCOVID 19 RadiologyДоржготов АриунболдNo ratings yet
- Imaging Coronavirus BSR ChestDocument29 pagesImaging Coronavirus BSR ChestGiulia LungulescuNo ratings yet
- Role of Imaging in Post Pnemumonia COVID-19Document22 pagesRole of Imaging in Post Pnemumonia COVID-19tenty isniNo ratings yet
- COVID19 PCP AIDS 2020 Case ReportDocument4 pagesCOVID19 PCP AIDS 2020 Case ReportmingNo ratings yet
- Time Course of Lung Changes at Chest CT During Recovery From Coronavirus Disease 2019 (COVID-19)Document7 pagesTime Course of Lung Changes at Chest CT During Recovery From Coronavirus Disease 2019 (COVID-19)Kykie KhongtokNo ratings yet
- Functional and Radiological Improvement in A COVID-19 Pneumonia Patient Treated With SteroidsDocument5 pagesFunctional and Radiological Improvement in A COVID-19 Pneumonia Patient Treated With Steroidsmostafa aliNo ratings yet
- Song, ImagenesDocument8 pagesSong, Imagenesismael yambayNo ratings yet
- Chest X-Ray Findings Monitoring COVID-19 Disease Course and SeverityDocument18 pagesChest X-Ray Findings Monitoring COVID-19 Disease Course and SeverityAdianto Tirta NugrahaNo ratings yet
- Nitra Piyavisetpat, MD Medpark Hospital King Chulalongkorn Memorial HospitalDocument42 pagesNitra Piyavisetpat, MD Medpark Hospital King Chulalongkorn Memorial HospitalSilp SatjawattanavimolNo ratings yet
- ImagingJurnal algorithm for COVID-19 detectionDocument29 pagesImagingJurnal algorithm for COVID-19 detectionIneke RomadinaNo ratings yet
- COVID-19 With Acute Cholecystitis: A Case: Casereport Open AccessDocument4 pagesCOVID-19 With Acute Cholecystitis: A Case: Casereport Open AccessMasithaNo ratings yet
- Performance of Radiologists in Differentiating COVID-19 From Non-COVID-19 Viral Pneumonia at Chest CTDocument9 pagesPerformance of Radiologists in Differentiating COVID-19 From Non-COVID-19 Viral Pneumonia at Chest CTrishaNo ratings yet
- Case Report JurnalDocument16 pagesCase Report JurnalAstrid PuspaNo ratings yet
- Sensitivity of Chest CT For COVID 19 Comparison To RT PCRDocument3 pagesSensitivity of Chest CT For COVID 19 Comparison To RT PCRkim niaNo ratings yet
- RRLDocument4 pagesRRLMUNDER OMAIRA NASRA D.No ratings yet
- BJR 20200219Document9 pagesBJR 20200219WilsonR.CorzoNiñoNo ratings yet
- Coronavirus (COVID-19) OutbreakDocument5 pagesCoronavirus (COVID-19) OutbreakPrima Sarana MedikaNo ratings yet
- Jurnal 20Document5 pagesJurnal 20Ahmad Fari Arief LopaNo ratings yet
- Clinico-Radiological Profile in Covid - 19 PatientsDocument6 pagesClinico-Radiological Profile in Covid - 19 PatientsInternational Journal of Innovative Science and Research Technology100% (1)
- Calon Jurnal Radio 1Document10 pagesCalon Jurnal Radio 1harryNo ratings yet
- Covid-19 Pneumonija Radioloska SlikaDocument11 pagesCovid-19 Pneumonija Radioloska SlikaStefan BaumanNo ratings yet
- Dynamics and Correlation Among Viral Positivity, Seroconversion, and Disease Severity in COVID-19Document15 pagesDynamics and Correlation Among Viral Positivity, Seroconversion, and Disease Severity in COVID-19yanuarizkaNo ratings yet
- Three Cases of COVID-19 Patients Presenting With Erythema: Concise CommunicationDocument4 pagesThree Cases of COVID-19 Patients Presenting With Erythema: Concise CommunicationNur Alfia KusumaningsihNo ratings yet
- Gambaran Hasil CT-Scan Toraks Pada Pasien Coronavirus Disease 2019 (COVID-19)Document6 pagesGambaran Hasil CT-Scan Toraks Pada Pasien Coronavirus Disease 2019 (COVID-19)rishaNo ratings yet
- Essentials For Radiologists OnDocument2 pagesEssentials For Radiologists Onzahra ebrahimiNo ratings yet
- 1 s2.0 S1930043320306208 MainDocument3 pages1 s2.0 S1930043320306208 MainRivaldy BobihuNo ratings yet
- 2019 Novel Coronavirus Disease (COVID-19) in Taiwan: Reports of Two Cases From Wuhan, ChinaDocument4 pages2019 Novel Coronavirus Disease (COVID-19) in Taiwan: Reports of Two Cases From Wuhan, ChinaClaav HugNo ratings yet
- Diagnosis and Treatment Plan of Corona Virus Disease 2019 (Tentative Sixth Edition)Document5 pagesDiagnosis and Treatment Plan of Corona Virus Disease 2019 (Tentative Sixth Edition)jameiNo ratings yet
- Clinical Progression of COVID-19 Patient With Extended Incubation Period, Delayed RT-PCR Time-To-Positivity, and Potential Role of Chest CT-scanDocument4 pagesClinical Progression of COVID-19 Patient With Extended Incubation Period, Delayed RT-PCR Time-To-Positivity, and Potential Role of Chest CT-scanSeri Agustin SartikaNo ratings yet
- Value of ICON in CoVid-19 Patients-2Document50 pagesValue of ICON in CoVid-19 Patients-2Mutiara PertiwiNo ratings yet
- COVID-19 Autopsies - Aqaa062Document9 pagesCOVID-19 Autopsies - Aqaa062Pramod BiradarNo ratings yet
- Jurnal 1Document5 pagesJurnal 1Jojo McalisterNo ratings yet
- Presumed Asymptomatic Carrier Transmission of COVID-19: MethodsDocument3 pagesPresumed Asymptomatic Carrier Transmission of COVID-19: MethodsChristine Jane RodriguezNo ratings yet
- Annals of Clinical Medicine and Research: Pulmonary Cavitation Post-COVID-19 Pneumonia: A CaseDocument3 pagesAnnals of Clinical Medicine and Research: Pulmonary Cavitation Post-COVID-19 Pneumonia: A CaseChavdarNo ratings yet
- Clinical Presentation of COVID-19: Case Series and Review of The LiteratureDocument11 pagesClinical Presentation of COVID-19: Case Series and Review of The LiteratureFaizzal AdmajaaNo ratings yet
- Positive Chest CT Features in Patients With COVID-19 Pneumonia and Negative Real-Time Polymerase Chain Reaction TestDocument16 pagesPositive Chest CT Features in Patients With COVID-19 Pneumonia and Negative Real-Time Polymerase Chain Reaction TestHector MarrufoNo ratings yet
- Rli 55 257Document5 pagesRli 55 257WilsonR.CorzoNiñoNo ratings yet
- Oral Candidiasis of COVID-19 Patients Case Report and ReviewDocument5 pagesOral Candidiasis of COVID-19 Patients Case Report and ReviewElizabeth SihiteNo ratings yet
- Disseminated Tuberculosis in An AIDS/HIV-Infected Patient: AbstractDocument3 pagesDisseminated Tuberculosis in An AIDS/HIV-Infected Patient: AbstractAmelia Fitria DewiNo ratings yet
- Correlation of Interferon Gamma (IFN-γ), Platelet to Lymphocyte Ratio (PLR), and Mortality of Covid-19 PatientsDocument4 pagesCorrelation of Interferon Gamma (IFN-γ), Platelet to Lymphocyte Ratio (PLR), and Mortality of Covid-19 PatientsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Correlation Between Ground-Glass Opacity On Pulmonary CT and The Levels of Inflammatory CytokinesDocument7 pagesCorrelation Between Ground-Glass Opacity On Pulmonary CT and The Levels of Inflammatory CytokinesEarlya RifaniNo ratings yet
- E001219 FullDocument2 pagesE001219 Fullayuni fatriciaNo ratings yet
- Low level immunoglobulinG (IgG) in reinfection case COVID-19 in BengkuluDocument4 pagesLow level immunoglobulinG (IgG) in reinfection case COVID-19 in BengkuluDebie RizqohNo ratings yet
- Calon Jurnal Radio 4Document7 pagesCalon Jurnal Radio 4harryNo ratings yet
- Wu2020 Article InterpretationOfCTSignsOf2019NDocument8 pagesWu2020 Article InterpretationOfCTSignsOf2019NBruce WilliamNo ratings yet
- Correlations of CT Scan With High-Sensitivity C-ReDocument5 pagesCorrelations of CT Scan With High-Sensitivity C-ReAnthony ChristantoNo ratings yet
- CT Scan Vs PCR2Document6 pagesCT Scan Vs PCR2risanataliasiburianNo ratings yet
- Bronchoscopy in Critically Ill COVID-19 Patients - Findings, Microbiological Profile, and CoinfectionDocument5 pagesBronchoscopy in Critically Ill COVID-19 Patients - Findings, Microbiological Profile, and CoinfectionJeisson Osorio TrujilloNo ratings yet
- Corona Virus Disease 2019, DHF and The Clinical SimilarityDocument3 pagesCorona Virus Disease 2019, DHF and The Clinical Similarityketut suryanaNo ratings yet
- Evaluation of Corona Virus Related Respiratory Illness by Chest Radiography at Tertiary Care Hospital, Agartala A Descriptive StudyDocument5 pagesEvaluation of Corona Virus Related Respiratory Illness by Chest Radiography at Tertiary Care Hospital, Agartala A Descriptive StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Radiol 2020200642Document9 pagesRadiol 2020200642sanya eusebia lupaca lupacaNo ratings yet
- COVID 19 Articulo MilordDocument11 pagesCOVID 19 Articulo MilordHector MartinezNo ratings yet
- Institutul National de Pneumoftiziologie Marius NastaDocument19 pagesInstitutul National de Pneumoftiziologie Marius NastaAlex PlaticaNo ratings yet
- REPORTE CASO TBC y COVID 19Document6 pagesREPORTE CASO TBC y COVID 19Farmaco VigilanciaNo ratings yet
- Chest X Ray Covid-19 DHSDocument52 pagesChest X Ray Covid-19 DHSBung SoeryNo ratings yet
- The War Against Covid-19 Pandemic: What Went Wrong? What Went Right? Losers And WinnersFrom EverandThe War Against Covid-19 Pandemic: What Went Wrong? What Went Right? Losers And WinnersNo ratings yet
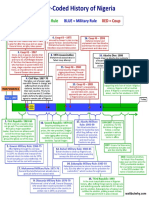
- Nigeria History3 PDFDocument1 pageNigeria History3 PDFViraj PanaraNo ratings yet
- Social distancing impact of COVID-19 in IndiaDocument9 pagesSocial distancing impact of COVID-19 in IndiaLouis RoderosNo ratings yet
- Advisory On Feasibility of Sample PoolingDocument1 pageAdvisory On Feasibility of Sample PoolingViraj PanaraNo ratings yet
- Advisory&Strategyfor Useof Rapid Antibody Based Blood TestDocument3 pagesAdvisory&Strategyfor Useof Rapid Antibody Based Blood TestViraj PanaraNo ratings yet
- Guidelines On Rational Use of PersonalProtectiveEquipmentDocument11 pagesGuidelines On Rational Use of PersonalProtectiveEquipmentchandan kumarNo ratings yet
- Containment Plan For Large Outbreaks: Novel Coronavirus Disease 2019 (COVID-19)Document20 pagesContainment Plan For Large Outbreaks: Novel Coronavirus Disease 2019 (COVID-19)Vijay SharmaNo ratings yet
- 03 12 2018 B PDFDocument11 pages03 12 2018 B PDFViraj PanaraNo ratings yet
- DAY-1 Placement Results for 38 CompaniesDocument4 pagesDAY-1 Placement Results for 38 CompaniesViraj PanaraNo ratings yet
- Covid 19 - Navigating The Uncharted NEJMe2002387 PDFDocument2 pagesCovid 19 - Navigating The Uncharted NEJMe2002387 PDFViraj PanaraNo ratings yet
- SARS-CoV2 Genome AnalysisDocument22 pagesSARS-CoV2 Genome AnalysisSMNo ratings yet
- Syllabus of INTRODUCTION TO EDUCATIONAL NEUROSCIENCEDocument3 pagesSyllabus of INTRODUCTION TO EDUCATIONAL NEUROSCIENCEViraj Panara100% (1)
- Papua New Guinea rice handbookDocument32 pagesPapua New Guinea rice handbookJoel WalgraeveNo ratings yet
- EthicsDocument18 pagesEthicsViraj PanaraNo ratings yet
- How To Write A Good Case StudyDocument7 pagesHow To Write A Good Case StudyJohn Patrick Atienza HillNo ratings yet
- Case Study TitanDocument11 pagesCase Study Titanmystique2sNo ratings yet
- Jung S Red Book An Old Book With New IdeasDocument66 pagesJung S Red Book An Old Book With New IdeasViraj Panara100% (1)
- Compare The Triplets EnglishDocument2 pagesCompare The Triplets EnglishViraj PanaraNo ratings yet
- Bhrigu SamhitaDocument2 pagesBhrigu Samhitajitnamp100% (1)
- Document From ANKITt1Document11 pagesDocument From ANKITt1Viraj PanaraNo ratings yet
- Samadhi - by Paramhansa Yogananda - Nayaswamis Jyotish and DeviDocument5 pagesSamadhi - by Paramhansa Yogananda - Nayaswamis Jyotish and DeviViraj PanaraNo ratings yet
- Compare The Triplets EnglishDocument2 pagesCompare The Triplets EnglishViraj PanaraNo ratings yet
- Affirmation PledgeDocument2 pagesAffirmation PledgeViraj PanaraNo ratings yet
- Compare The Triplets EnglishDocument2 pagesCompare The Triplets EnglishViraj PanaraNo ratings yet
- ch4 PDFDocument31 pagesch4 PDFkrunal07786No ratings yet
- Ges 2k17 Quiz-O-PreneurDocument5 pagesGes 2k17 Quiz-O-PreneurViraj PanaraNo ratings yet
- ANE BelakangDocument3 pagesANE BelakangGustomo PanantroNo ratings yet
- The Advantages and Disadvantages of Smart CitiesDocument3 pagesThe Advantages and Disadvantages of Smart CitiesthuantethiNo ratings yet
- Stroke Prediction System Using ANN (Artificial Neural Network)Document3 pagesStroke Prediction System Using ANN (Artificial Neural Network)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Private Health Institutions LawDocument22 pagesPrivate Health Institutions LawShankar SanyalNo ratings yet
- Factorial Design Fiction ManuscriptDocument5 pagesFactorial Design Fiction Manuscriptdave_scribedNo ratings yet
- Treat Chronic DacryocystitisDocument34 pagesTreat Chronic DacryocystitisAriyanie NurtaniaNo ratings yet
- UKFP 2024 Applicant HandbookDocument20 pagesUKFP 2024 Applicant HandbookS Abi GunnamNo ratings yet
- AmenorrheaDocument41 pagesAmenorrheadoraNo ratings yet
- MSCDFSM Prog. GuideDocument108 pagesMSCDFSM Prog. Guidesamraju1No ratings yet
- Dysfunctional Uterine Bleeding History CollectionDocument4 pagesDysfunctional Uterine Bleeding History CollectionAnitha BalakrishnanNo ratings yet
- Article+0202 368 379Document12 pagesArticle+0202 368 379Muhammad Alif Nur FaizinNo ratings yet
- Martindale drug reference 38th edition downloadDocument3 pagesMartindale drug reference 38th edition downloadChristian SosaNo ratings yet
- Self-Learning Module For Grade 11Document5 pagesSelf-Learning Module For Grade 11Joy S. CalayoNo ratings yet
- Case 2 Fery-1Document4 pagesCase 2 Fery-1Fery WiraNo ratings yet
- HTM 01 01 PartADocument59 pagesHTM 01 01 PartAwaseem kausarNo ratings yet
- Self-Assessment of Nursing Standards of PracticeDocument32 pagesSelf-Assessment of Nursing Standards of Practiceapi-242114301No ratings yet
- Lesson 52ND Q ManifestoDocument30 pagesLesson 52ND Q ManifestoLiya Mae SantiagoNo ratings yet
- Cariogram E BookDocument90 pagesCariogram E BookAlifianNo ratings yet
- THE ETHICS OF PUBLIC HEALTH SURVEILLANCE MCQsDocument2 pagesTHE ETHICS OF PUBLIC HEALTH SURVEILLANCE MCQsChaman Lal Karotia100% (1)
- Movie Review - Psychological Disorder PortrayedDocument3 pagesMovie Review - Psychological Disorder Portrayedwebster080808No ratings yet
- Clinical Pharmacy Thesis TopicsDocument6 pagesClinical Pharmacy Thesis Topicsbsk561ek100% (2)
- History of CounsellingDocument7 pagesHistory of Counsellingsam sangeethNo ratings yet
- AlzheimersDocument9 pagesAlzheimersNader Smadi100% (1)
- Resin Manufacturing EIA ReportDocument69 pagesResin Manufacturing EIA ReportNitin PatelNo ratings yet