You might also like
- Specimen Collection and Processing For Hemostasis TestingDocument22 pagesSpecimen Collection and Processing For Hemostasis TestingTom Anthony Tonguia100% (1)
- Wintrobe Test PDFDocument9 pagesWintrobe Test PDFMaria Chacón CarbajalNo ratings yet
- Capillary Fragility/ Resistance Test: Tourniquet or Rumpel-Leede or Hess TestDocument4 pagesCapillary Fragility/ Resistance Test: Tourniquet or Rumpel-Leede or Hess TestGerly MaglangitNo ratings yet
- Intro To ImmunohematoDocument48 pagesIntro To Immunohematojong188No ratings yet
- Chapter Blood: RBC Platelet HemostasisDocument89 pagesChapter Blood: RBC Platelet Hemostasisapi-19916399100% (1)
- LABORATORY MEASUREMENTS OF PLATELET ACTIVITIESDocument73 pagesLABORATORY MEASUREMENTS OF PLATELET ACTIVITIESMary Lyka ReyesNo ratings yet
- Gel TechnologyDocument2 pagesGel TechnologyJai Carungay100% (1)
- COMPLETE BLOOD COUNT Lecture GuideDocument9 pagesCOMPLETE BLOOD COUNT Lecture GuideKaycee Gretz LorescaNo ratings yet
- Serological TestsDocument2 pagesSerological TestsKimberly EspaldonNo ratings yet
- HemaDocument59 pagesHemaSteph VeeNo ratings yet
- Hematology II Notes - MagtalasDocument12 pagesHematology II Notes - MagtalasAbhugz VosotrosNo ratings yet
- Routine Laboratory Evaluation of CoagulationDocument32 pagesRoutine Laboratory Evaluation of CoagulationArshie08No ratings yet
- Lec 9-10 Blood Groups & TransfusionDocument51 pagesLec 9-10 Blood Groups & TransfusionEmily Peterson100% (1)
- Autoimmune Hemolytic AnemiaDocument55 pagesAutoimmune Hemolytic AnemiaNicky SebastianNo ratings yet
- Clotting Time TestDocument2 pagesClotting Time TestÕmodëlë Åresa RöbinsonNo ratings yet
- University of Santo Tomas Immunohematology and Transfusion MedicineDocument7 pagesUniversity of Santo Tomas Immunohematology and Transfusion MedicineWynlor Abarca100% (1)
- Hematology 2 TEST QUESTIONSDocument4 pagesHematology 2 TEST QUESTIONSa a r o n b a u t i s t aNo ratings yet
- Blood BankingDocument7 pagesBlood BankingRoiland Atienza BaybayonNo ratings yet
- Renal Anatomy & Physiology OverviewDocument5 pagesRenal Anatomy & Physiology OverviewChristopher BucuNo ratings yet
- Vascular System Vascular Structure and FunctionDocument8 pagesVascular System Vascular Structure and FunctionEriq BaldovinoNo ratings yet
- Immuno HematologyDocument35 pagesImmuno HematologyAlan McLeanNo ratings yet
- HaematologyDocument68 pagesHaematologytapoolnoNo ratings yet
- Blood Banking Course BookDocument2 pagesBlood Banking Course BookShukr Wesman BlbasNo ratings yet
- Lab Evaluation of PlateletsDocument5 pagesLab Evaluation of PlateletsDennis ValdezNo ratings yet
- Hematology Services GuideDocument34 pagesHematology Services GuideLorelie CarlosNo ratings yet
- Blood Bank QuizDocument13 pagesBlood Bank Quizdimalawang.af100% (1)
- Urine Specimen Collection: Ms. Sneha SehrawatDocument36 pagesUrine Specimen Collection: Ms. Sneha SehrawatRajaNo ratings yet
- Compatibility Testing - BloodDocument5 pagesCompatibility Testing - BloodMunish DograNo ratings yet
- Hematology2 - Laboratory TestsDocument3 pagesHematology2 - Laboratory Testskthmnts100% (1)
- Blood Smear Examination 1معدل Document74 pagesBlood Smear Examination 1معدل Kenesa100% (1)
- Manual Platelet CountDocument14 pagesManual Platelet CountMiyo SobremisanaNo ratings yet
- Coagulation CascadeDocument4 pagesCoagulation CascadezainabNo ratings yet
- Component Therapy-Transfusion of TheDocument8 pagesComponent Therapy-Transfusion of TheGennelyn Ross Delos ReyesNo ratings yet
- 1335687089.75523 Lab PracticalHematologyManualDocument62 pages1335687089.75523 Lab PracticalHematologyManualAgustín Manriquez EspinozaNo ratings yet
- Platelet CountDocument2 pagesPlatelet CountSirias_black100% (2)
- PlateletsDocument23 pagesPlateletsnirilibNo ratings yet
- Disorders of Coagulation and Thrombosis NotesDocument16 pagesDisorders of Coagulation and Thrombosis NotesleeNo ratings yet
- C1 IH Lab L3 ABO Forward Reverse Typing Manual and Gel MethodDocument8 pagesC1 IH Lab L3 ABO Forward Reverse Typing Manual and Gel MethodDIVINA KYLE YGONo ratings yet
- Joshua Ty Cayetano 3DMT #15: A B C A B B B A ADocument4 pagesJoshua Ty Cayetano 3DMT #15: A B C A B B B A AJoshua Ty CayetanoNo ratings yet
- Blood Bank TypingDocument34 pagesBlood Bank TypingSkylarNo ratings yet
- Group 6 - Immunohematology - Blood BankingDocument8 pagesGroup 6 - Immunohematology - Blood Bankingjulo_05No ratings yet
- PlateletDocument15 pagesPlateletFafha FafhaNo ratings yet
- Top 10 Anemias to Know for BoardsDocument24 pagesTop 10 Anemias to Know for BoardsSim M ChangNo ratings yet
- Donor Selection and Blood CollectionDocument14 pagesDonor Selection and Blood CollectionMary ChristelleNo ratings yet
- CBC Reviewer Anaphy LabDocument9 pagesCBC Reviewer Anaphy LabARVINE JUSTINE CORPUZNo ratings yet
- Hematology 1 Lab - The Reticulocyte CountDocument17 pagesHematology 1 Lab - The Reticulocyte CountCIRILO MABBORANGNo ratings yet
- Blood Groups & Blood BankingDocument36 pagesBlood Groups & Blood BankingGodfrey Pizaroh Mujuzi100% (2)
- Clearance and GFR: Major DR Arabinda Mohan Bhattarai Lecturer (Biochemistry), NAIHSDocument25 pagesClearance and GFR: Major DR Arabinda Mohan Bhattarai Lecturer (Biochemistry), NAIHSChandan SahNo ratings yet
- Bleeding Time Test ExplainedDocument9 pagesBleeding Time Test ExplainedHendra SshNo ratings yet
- Compatibility Testing: Week 5Document33 pagesCompatibility Testing: Week 5Bridgette100% (1)
- Gram Positive CocciDocument34 pagesGram Positive CocciMaria Cecilia Flores50% (2)
- Blood BankDocument84 pagesBlood Bankmanni1001100% (4)
- Hematology Lecture Notes for Medical StudentsDocument88 pagesHematology Lecture Notes for Medical StudentsharpreetNo ratings yet
- Hema Ii Laboratory Week 6Document65 pagesHema Ii Laboratory Week 6Al-hadad AndromacheNo ratings yet
- Antibody IdentificationDocument27 pagesAntibody Identificationhamaada100% (1)
- Donor Screening and Component PreparationDocument91 pagesDonor Screening and Component PreparationDominic BernardoNo ratings yet
- Agglutination, Complement, Neutralization, and Inhibition: Methods in Immunology and Immunochemistry, Vol. 4From EverandAgglutination, Complement, Neutralization, and Inhibition: Methods in Immunology and Immunochemistry, Vol. 4No ratings yet
- The Learning EnvironmentDocument25 pagesThe Learning EnvironmentTom Anthony TonguiaNo ratings yet
- Quality Management in Blood BankingDocument17 pagesQuality Management in Blood BankingTom Anthony TonguiaNo ratings yet
- Data On Patients Having StomachDocument1 pageData On Patients Having StomachTom Anthony TonguiaNo ratings yet
- Safety and Clinical Management in Clinical Microscopy SectionDocument21 pagesSafety and Clinical Management in Clinical Microscopy SectionTom Anthony TonguiaNo ratings yet
- CellDocument27 pagesCellTom Anthony TonguiaNo ratings yet
- Course Syllabus - CPH LabDocument2 pagesCourse Syllabus - CPH LabTom Anthony TonguiaNo ratings yet
- Basic Apparatus and Equipment in MicrobiologyDocument10 pagesBasic Apparatus and Equipment in MicrobiologyTom Anthony TonguiaNo ratings yet
- Case-Study-HISTO LAB EDLAY2ADocument2 pagesCase-Study-HISTO LAB EDLAY2ATom Anthony TonguiaNo ratings yet
- PortfolioDocument2 pagesPortfolioTom Anthony TonguiaNo ratings yet
- Orca Share Media1592386429020 6678952768787381131Document3 pagesOrca Share Media1592386429020 6678952768787381131Tom Anthony TonguiaNo ratings yet
- Rubrics For EssayDocument2 pagesRubrics For EssayTom Anthony TonguiaNo ratings yet
- Orca Share Media1592386429033 6678952768839356579Document2 pagesOrca Share Media1592386429033 6678952768839356579Tom Anthony TonguiaNo ratings yet
- Journal of Clinical Microbiology-2020-Theel-JCM.01243-20.fullDocument23 pagesJournal of Clinical Microbiology-2020-Theel-JCM.01243-20.fullTom Anthony TonguiaNo ratings yet
- Activity 2 Finals Histo Lab - EDLAY2ADocument2 pagesActivity 2 Finals Histo Lab - EDLAY2ATom Anthony TonguiaNo ratings yet
- Cell Division (Mitosis & Meiosis)Document8 pagesCell Division (Mitosis & Meiosis)Tom Anthony TonguiaNo ratings yet
- Tom Anthony A. Tonguia, RMTDocument1 pageTom Anthony A. Tonguia, RMTTom Anthony TonguiaNo ratings yet
- Orca Share Media1592386428992 6678952768667573458Document2 pagesOrca Share Media1592386428992 6678952768667573458Tom Anthony TonguiaNo ratings yet
- By: Tom Anthony A. Tonguia, RMT: Eukaryotic CellDocument9 pagesBy: Tom Anthony A. Tonguia, RMT: Eukaryotic CellTom Anthony TonguiaNo ratings yet
- Quiz 1 (Histo Lab)Document6 pagesQuiz 1 (Histo Lab)Tom Anthony TonguiaNo ratings yet
- Muscle and Nervous TissueDocument12 pagesMuscle and Nervous TissueTom Anthony TonguiaNo ratings yet
- Quiz 3Document5 pagesQuiz 3Tom Anthony TonguiaNo ratings yet
- Muscle and Nervous TissueDocument12 pagesMuscle and Nervous TissueTom Anthony TonguiaNo ratings yet
- Histology Lab Techniques GuideDocument16 pagesHistology Lab Techniques GuideTom Anthony TonguiaNo ratings yet
- Epithelial TissueDocument40 pagesEpithelial TissueTom Anthony TonguiaNo ratings yet
- Connective Tissues: Support, Anchor and Connect the BodyDocument7 pagesConnective Tissues: Support, Anchor and Connect the BodyTom Anthony TonguiaNo ratings yet
- By: Tom Anthony A. Tonguia, RMT: Eukaryotic CellDocument9 pagesBy: Tom Anthony A. Tonguia, RMT: Eukaryotic CellTom Anthony TonguiaNo ratings yet
- WBC DifferentiationDocument5 pagesWBC DifferentiationTom Anthony TonguiaNo ratings yet
- Cell Division (Mitosis & Meiosis)Document8 pagesCell Division (Mitosis & Meiosis)Tom Anthony TonguiaNo ratings yet
- Hema Lec Catch Up Plan FinalsDocument2 pagesHema Lec Catch Up Plan FinalsTom Anthony TonguiaNo ratings yet
- 11.histo Digestive SystemDocument92 pages11.histo Digestive SystemTom Anthony TonguiaNo ratings yet
- Komplikasi Dan Indikasi Transfusi DarahDocument24 pagesKomplikasi Dan Indikasi Transfusi DarahwelNo ratings yet
- Reovirus - RotavirusDocument13 pagesReovirus - Rotaviruszakiyyatul aflakhaNo ratings yet
- Sindroamele HemoragiceDocument5 pagesSindroamele HemoragiceIoana GalNo ratings yet
- Chapter Review: True or FalseDocument2 pagesChapter Review: True or FalseJames Gabriel SalardaNo ratings yet
- Hematology QuizDocument7 pagesHematology Quizsanwel80% (5)
- Practical 1 Lab Report BIO301 PDFDocument5 pagesPractical 1 Lab Report BIO301 PDFfar50% (2)
- Micro Lab ReportDocument5 pagesMicro Lab Reportrdover83% (6)
- Approach To The Child With Anemia - UpToDateDocument41 pagesApproach To The Child With Anemia - UpToDateDaniel Enrique CardenasNo ratings yet
- Blood Group SystemDocument5 pagesBlood Group SystemSAMEER KUMARNo ratings yet
- Pathognomonic Signs of Communicable Diseases: JJ8009 Health & NutritionDocument2 pagesPathognomonic Signs of Communicable Diseases: JJ8009 Health & NutritionMauliza Resky NisaNo ratings yet
- Curriculum VitaeDocument6 pagesCurriculum Vitaezeleke100% (1)
- Undangan Sepsis 24 Nov 2018 1st AnnDocument2 pagesUndangan Sepsis 24 Nov 2018 1st AnnAtik Marfu'ahNo ratings yet
- Etest Brochure 1Document2 pagesEtest Brochure 1Nidia MaradiagaNo ratings yet
- Bovine Serum Albumin 22%Document1 pageBovine Serum Albumin 22%Sameeh MohNo ratings yet
- The Role of Vaccination in Salmonella ControlDocument51 pagesThe Role of Vaccination in Salmonella ControlDr. Aja Ogboo Chikere100% (1)
- Teknis Identifikasi Jamur Biakan IdentifikasiDocument47 pagesTeknis Identifikasi Jamur Biakan IdentifikasiSo FunnNo ratings yet
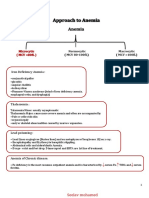
- Normocytic and Macrocytic Anemia Causes and SymptomsDocument4 pagesNormocytic and Macrocytic Anemia Causes and SymptomspNo ratings yet
- Microbiology SyllabusDocument2 pagesMicrobiology Syllabusapi-3704804No ratings yet
- Aso (Antistreptolysin O) PDFDocument3 pagesAso (Antistreptolysin O) PDFIbrahim SiddigNo ratings yet
- Authorize blood donation card use for spouse transfusionDocument1 pageAuthorize blood donation card use for spouse transfusionQC TownhomesNo ratings yet
- Immunohema & Transfusion MedDocument62 pagesImmunohema & Transfusion MedMark Joseph Felicitas CuntapayNo ratings yet
- E.M.B. Levine Agar: Typical Formula (G/L)Document2 pagesE.M.B. Levine Agar: Typical Formula (G/L)Mitha AriantiNo ratings yet
- Lab RXDocument1 pageLab RXRURAL HEALTH CENTER TAMBLER BAWINGNo ratings yet
- Transfusion of Apheresis Platelets and Abo Groups 2005Document15 pagesTransfusion of Apheresis Platelets and Abo Groups 2005my accountNo ratings yet
- Culture Media Classification and Uses in 40 CharactersDocument9 pagesCulture Media Classification and Uses in 40 CharactersAhsan AhmadNo ratings yet
- MRS Broth: (Lactosebacillus Broth Acc. To DE MAN, ROGOSA and SHARPE)Document1 pageMRS Broth: (Lactosebacillus Broth Acc. To DE MAN, ROGOSA and SHARPE)Aswina NadiaNo ratings yet
- Platelet Function TestsDocument27 pagesPlatelet Function TestsTusabe FredNo ratings yet
- Microbiology Module 7 - BacilliDocument87 pagesMicrobiology Module 7 - BacilliArt Arts100% (1)
- Morning Report Pediatric DepartmentDocument18 pagesMorning Report Pediatric DepartmentMedina MarwanNo ratings yet
- National Microbiology Quiz Organised by Nanyang Polytechnic & SSMBDocument3 pagesNational Microbiology Quiz Organised by Nanyang Polytechnic & SSMBSamuel FongNo ratings yet