You might also like
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- What Is A Bone Marrow Transplant?Document4 pagesWhat Is A Bone Marrow Transplant?Krisna AgustiniNo ratings yet
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesFrom EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesNo ratings yet
- Bone Marrow TransplantDocument8 pagesBone Marrow TransplantPSRI hospitalNo ratings yet
- 17 ManuscriptDocument10 pages17 ManuscriptBaru Chandrasekhar RaoNo ratings yet
- Carcinoma of TongueDocument51 pagesCarcinoma of Tonguesri wulan dhariNo ratings yet
- Lip Cancer-Ablative and Reconstructive Surgery: ChapDocument52 pagesLip Cancer-Ablative and Reconstructive Surgery: ChapYang Lin Chen100% (1)
- Streptokinase GroupDocument16 pagesStreptokinase GroupSuffocated LiveNo ratings yet
- UrethritisDocument11 pagesUrethritismarej143No ratings yet
- Nursing College Address Etc.Document4 pagesNursing College Address Etc.ParvezNo ratings yet
- Antiretroviral DrugsDocument60 pagesAntiretroviral DrugsDeribe BekeleNo ratings yet
- Chikungunya FeverDocument15 pagesChikungunya FeverAyomide AlayandeNo ratings yet
- Wound AssessmentDocument19 pagesWound Assessmentdrsonuchawla100% (1)
- Manteux TestDocument25 pagesManteux TestEvaNatashaNo ratings yet
- Oxaliplatin Monograph 1dec2016Document9 pagesOxaliplatin Monograph 1dec2016Nadial UzmahNo ratings yet
- Understanding Hepatic Encephalopathy (HE) Symptoms, Causes and TreatmentDocument3 pagesUnderstanding Hepatic Encephalopathy (HE) Symptoms, Causes and TreatmentSuhas KandeNo ratings yet
- Chymoral PlusDocument3 pagesChymoral PlusNeha SureshNo ratings yet
- 11 Nursing Management in Uterine (Endometrial) CancerDocument17 pages11 Nursing Management in Uterine (Endometrial) Cancerclaire yowsNo ratings yet
- Intravenous Fluid Therapy: Types and UsesDocument11 pagesIntravenous Fluid Therapy: Types and UsesHayashi Breads MaaNo ratings yet
- AdrenalineDocument2 pagesAdrenalinerazvan032006100% (1)
- HIV Treatment 2Document3 pagesHIV Treatment 2kimglaidyl bontuyanNo ratings yet
- NEW ZEALAND DATA SHEET PETHIDINE TABLETSDocument13 pagesNEW ZEALAND DATA SHEET PETHIDINE TABLETSAnonymous NQDRERPcjNo ratings yet
- Heparin LitigationDocument34 pagesHeparin LitigationjvalgalNo ratings yet
- Briviact Film-Coated Tablets Summary of Product CharacteristicsDocument110 pagesBriviact Film-Coated Tablets Summary of Product CharacteristicsBendisDacicaNo ratings yet
- Vincristine MonographDocument9 pagesVincristine MonographcmeytasNo ratings yet
- Idiopathic Thrombocytopenic Purpura: Overview With Report of A CaseDocument4 pagesIdiopathic Thrombocytopenic Purpura: Overview With Report of A CaseHernan GonzalezNo ratings yet
- Biliary DyskinesiaDocument1 pageBiliary DyskinesiaYolotl Hilario Sanchez CarrilloNo ratings yet
- Fulminant Hepatic FailureDocument12 pagesFulminant Hepatic Failureafghansyah arfiantoNo ratings yet
- Esophageal Carcinoma Anatomy, Symptoms, Risk FactorsDocument5 pagesEsophageal Carcinoma Anatomy, Symptoms, Risk FactorsChiu ChunNo ratings yet
- Management of Pregnancy JaundiceDocument28 pagesManagement of Pregnancy JaundiceShailani Thakur100% (1)
- Central Venous Access Devices (Cvads)Document40 pagesCentral Venous Access Devices (Cvads)DocRNNo ratings yet
- Managing Nause and Vomiting-Crit-Care-Nurse-2003-Garrett-31-50 PDFDocument22 pagesManaging Nause and Vomiting-Crit-Care-Nurse-2003-Garrett-31-50 PDFpmuftiaNo ratings yet
- Purpura and Petechiae: Symptoms and Types of Idiopathic Thrombocytopenic Purpura (ITPDocument7 pagesPurpura and Petechiae: Symptoms and Types of Idiopathic Thrombocytopenic Purpura (ITPMarie Joe AbainzaNo ratings yet
- Lumbar Disc HerniationDocument19 pagesLumbar Disc HerniationPutri WulandariNo ratings yet
- Pneumonia Management ProtocolDocument2 pagesPneumonia Management Protocolsky nuts100% (1)
- Anti-Malarial DrugsDocument58 pagesAnti-Malarial Drugs88AKKNo ratings yet
- Bone Marrow TransplantDocument6 pagesBone Marrow TransplantFatihah UmerNo ratings yet
- Vesicovaginal FistulaDocument6 pagesVesicovaginal FistulaMaiza TusiminNo ratings yet
- Steps To Perform A Blood TransfusionDocument1 pageSteps To Perform A Blood Transfusionzepoli_zepoly6232No ratings yet
- Sick Sinus Syndrome 1Document23 pagesSick Sinus Syndrome 1Salman HabeebNo ratings yet
- Failure To ThriveDocument2 pagesFailure To Thrivekafosid100% (1)
- Folic Acid Presentation PDFDocument13 pagesFolic Acid Presentation PDFAngela IlustrisimoNo ratings yet
- Assessment of PainDocument4 pagesAssessment of PaingwapdoseNo ratings yet
- Transurethral Resection of the Prostate (TURP) ExplainedDocument23 pagesTransurethral Resection of the Prostate (TURP) ExplainedColeen Comelle HuertoNo ratings yet
- HIV and Its TreatmentDocument24 pagesHIV and Its Treatmentaathira_kNo ratings yet
- Clinical Case On JaundiceDocument43 pagesClinical Case On JaundicePro fatherNo ratings yet
- Nasogastric Tube FeedingDocument4 pagesNasogastric Tube FeedingAru VermaNo ratings yet
- Malaria: Dr. Shree Narayan Yadav Internal Medicine Resident NamsDocument40 pagesMalaria: Dr. Shree Narayan Yadav Internal Medicine Resident Namsasyanadhikary18No ratings yet
- Esophageal CancerDocument40 pagesEsophageal Cancerapi-282115150No ratings yet
- Chemotherapeutic DrugsDocument4 pagesChemotherapeutic DrugsEditor IJTSRDNo ratings yet
- Acute Lymphoblastic LeukemiaDocument34 pagesAcute Lymphoblastic LeukemiamtyboyNo ratings yet
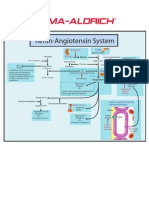
- Renin-Angiotensin SystemDocument1 pageRenin-Angiotensin SystemSigma-Aldrich100% (2)
- Anticancer Drugs: Consumer ChemistryDocument24 pagesAnticancer Drugs: Consumer ChemistryAshlie AbalaNo ratings yet
- Periampullary TumorsDocument30 pagesPeriampullary TumorsAsif.N.IqbalNo ratings yet
- Mesalazine: Mesalazine (INN, BAN), Also Known As Mesalamine (USAN) or 5-Aminosalicylic AcidDocument4 pagesMesalazine: Mesalazine (INN, BAN), Also Known As Mesalamine (USAN) or 5-Aminosalicylic AcidAnkan PalNo ratings yet
- Family Nursing Care PlanDocument11 pagesFamily Nursing Care PlanLester_Serrano_8967No ratings yet
- RBC AliquotsDocument1 pageRBC AliquotsARIF AHAMMEDNo ratings yet
- PancreatitisDocument12 pagesPancreatitismardsz100% (5)
- Day 2 - Ulcerative Colitis PDFDocument14 pagesDay 2 - Ulcerative Colitis PDFMaria Charis Anne IndananNo ratings yet
- How To InstallDocument2 pagesHow To InstallChristian De GuzmanNo ratings yet
- NCP Acute Pain PDFDocument3 pagesNCP Acute Pain PDFChristian De GuzmanNo ratings yet
- NCP-Risk For InfectionDocument2 pagesNCP-Risk For InfectionJea Joel Mendoza100% (1)
- T104 - TM Style Guide - Version 2.0 Reva PDFDocument39 pagesT104 - TM Style Guide - Version 2.0 Reva PDFAntoniaNo ratings yet
- Transcribe ExamDocument14 pagesTranscribe ExamAndreea Pop100% (1)
- HEPATITIS A AND B: SIGNS, SYMPTOMS, AND TREATMENTDocument18 pagesHEPATITIS A AND B: SIGNS, SYMPTOMS, AND TREATMENTChristian De GuzmanNo ratings yet
- NCP Acute PainDocument3 pagesNCP Acute PainChristian De GuzmanNo ratings yet
- 2015 Book IntroductionToNursingInformatiDocument456 pages2015 Book IntroductionToNursingInformatiChristian De GuzmanNo ratings yet
- Intestinal Telescoping in Children Under 1Document1 pageIntestinal Telescoping in Children Under 1Christian De GuzmanNo ratings yet
- Severe Acute MalnutritionDocument4 pagesSevere Acute MalnutritionAlemayehu DargeNo ratings yet
- Internship Report Asma EshanDocument40 pagesInternship Report Asma Eshanm bilalNo ratings yet
- IMNCI Management of Childhood Illness Chart Booklet WHO 2018Document54 pagesIMNCI Management of Childhood Illness Chart Booklet WHO 2018IgweNo ratings yet
- Evidences Plumpy DozDocument2 pagesEvidences Plumpy DozBassel MhannaNo ratings yet
- Underweight and MalnutritionDocument61 pagesUnderweight and MalnutritionJack Sinaga100% (1)
- CMAM Training PPT 2018 - 0Document57 pagesCMAM Training PPT 2018 - 0cabdinuux32No ratings yet
- Protein-Energy MalnutritionDocument6 pagesProtein-Energy MalnutritionSophy ChelotiNo ratings yet
- Ready To Use Therapeutic Food in RwandaDocument25 pagesReady To Use Therapeutic Food in RwandaKABERA RENENo ratings yet
- Module 8c-MNDC MNP in CMAM SiteDocument39 pagesModule 8c-MNDC MNP in CMAM SiteAliyu sa'aduNo ratings yet
- IMAM Guidelines For Uganda Jan2016 PDFDocument204 pagesIMAM Guidelines For Uganda Jan2016 PDFkamakyageofrey100% (3)
- Nutritional Rehabilitation: Presented By: Dr. Kunal Guided By: Dr. Abhay MudeyDocument43 pagesNutritional Rehabilitation: Presented By: Dr. Kunal Guided By: Dr. Abhay MudeyNazia Arif100% (1)
- GOS CMAM IC Mod1 Introduction Nov2011Document29 pagesGOS CMAM IC Mod1 Introduction Nov2011Nensy AnggrainyNo ratings yet
- Formula Terapeutica Lista para ConsumoDocument9 pagesFormula Terapeutica Lista para Consumo860707No ratings yet
- Peanuts As Functional Food: A ReviewDocument28 pagesPeanuts As Functional Food: A ReviewLPATI12No ratings yet
- UNICEF Ready-To-use Therapeutic Food Current OutlookDocument9 pagesUNICEF Ready-To-use Therapeutic Food Current OutlooksaiNo ratings yet
- Nutritional Status of Internally Displaced Children As Percieved by Mothers in Fisheries Buru-Un and Sagonsongan Marawi Evacuation CentersDocument26 pagesNutritional Status of Internally Displaced Children As Percieved by Mothers in Fisheries Buru-Un and Sagonsongan Marawi Evacuation CentersNorhaniah AmerNo ratings yet
- Nourishing People Feeding HopeDocument90 pagesNourishing People Feeding HopeKristin AvsiNo ratings yet
- Formulations For Fortified Complementary Foods and Supplements: Review of Successful Products For Improving The Nutritional Status of Infants and Young ChildrenDocument17 pagesFormulations For Fortified Complementary Foods and Supplements: Review of Successful Products For Improving The Nutritional Status of Infants and Young ChildrenDinesh SenathipathiNo ratings yet
- DOH Devolution Transition Plan 2022-2024Document45 pagesDOH Devolution Transition Plan 2022-2024An Di100% (1)
- Module 4Document107 pagesModule 4roseannurakNo ratings yet
- WHO Guidelines On Acute Malnutrition, 2023Document188 pagesWHO Guidelines On Acute Malnutrition, 2023Arafat HassanNo ratings yet
- Jurnal Utk Mengerjakan Soal No 1Document11 pagesJurnal Utk Mengerjakan Soal No 1Anny Nila SyauqiyyahNo ratings yet
- Kwashiorkor AND Marasmus: Group 6Document18 pagesKwashiorkor AND Marasmus: Group 6Christian De GuzmanNo ratings yet
- 2015 March 11 Peanut ReviewDocument28 pages2015 March 11 Peanut ReviewEmmanuel AbonNo ratings yet
- U.S. Fund For UNICEF Annual Report 2008Document19 pagesU.S. Fund For UNICEF Annual Report 2008U.S. Fund for UNICEFNo ratings yet
- Nutritional Interventions During Adolescence and Their Possible EffectsDocument23 pagesNutritional Interventions During Adolescence and Their Possible EffectsWalter MendozaNo ratings yet
- CMAM Training PPT 2018 - 0Document57 pagesCMAM Training PPT 2018 - 0معلومة كيميائيةNo ratings yet
- Namibia Flipchart Algorithm Child Sep2010Document11 pagesNamibia Flipchart Algorithm Child Sep2010Gabriela Morante RuizNo ratings yet
- Community Based Management of Acute MalnutritionDocument149 pagesCommunity Based Management of Acute MalnutritionGirma Goshime100% (2)
- Nutrition Intervention to Reduce MalnutritionDocument31 pagesNutrition Intervention to Reduce MalnutritionJosephNo ratings yet
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyFrom EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyRating: 5 out of 5 stars5/5 (1)
- Love Yourself, Heal Your Life Workbook (Insight Guide)From EverandLove Yourself, Heal Your Life Workbook (Insight Guide)Rating: 5 out of 5 stars5/5 (40)
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeFrom EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- Forever Strong: A New, Science-Based Strategy for Aging WellFrom EverandForever Strong: A New, Science-Based Strategy for Aging WellNo ratings yet
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookFrom EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookRating: 3.5 out of 5 stars3.5/5 (2)
- The Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingFrom EverandThe Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingRating: 4 out of 5 stars4/5 (3)
- Body Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomFrom EverandBody Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomRating: 4 out of 5 stars4/5 (1)
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisFrom EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisRating: 3 out of 5 stars3/5 (2)
- The Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyFrom EverandThe Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyNo ratings yet
- Summary of Mary Claire Haver's The Galveston DietFrom EverandSummary of Mary Claire Haver's The Galveston DietRating: 5 out of 5 stars5/5 (1)
- Find Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeFrom EverandFind Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeRating: 4 out of 5 stars4/5 (3)
- The Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonFrom EverandThe Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonRating: 3.5 out of 5 stars3.5/5 (33)
- The Stark Naked 21-Day Metabolic Reset: Effortless Weight Loss, Rejuvenating Sleep, Limitless Energy, More MojoFrom EverandThe Stark Naked 21-Day Metabolic Reset: Effortless Weight Loss, Rejuvenating Sleep, Limitless Energy, More MojoNo ratings yet
- Happy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainFrom EverandHappy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainRating: 3.5 out of 5 stars3.5/5 (6)
- Secrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainFrom EverandSecrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainRating: 3.5 out of 5 stars3.5/5 (38)
- The Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsFrom EverandThe Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsRating: 4 out of 5 stars4/5 (49)
- Sugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthFrom EverandSugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthRating: 4 out of 5 stars4/5 (6)
- Glucose Goddess Method: A 4-Week Guide to Cutting Cravings, Getting Your Energy Back, and Feeling AmazingFrom EverandGlucose Goddess Method: A 4-Week Guide to Cutting Cravings, Getting Your Energy Back, and Feeling AmazingRating: 5 out of 5 stars5/5 (60)
- Keto Friendly Recipes: Easy Keto For Busy PeopleFrom EverandKeto Friendly Recipes: Easy Keto For Busy PeopleRating: 3.5 out of 5 stars3.5/5 (2)
- The Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthFrom EverandThe Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthNo ratings yet
- Allen Carr's Easy Way for Women to Lose Weight: The original Easyway methodFrom EverandAllen Carr's Easy Way for Women to Lose Weight: The original Easyway methodRating: 4.5 out of 5 stars4.5/5 (18)
- Glucose Revolution: The Life-Changing Power of Balancing Your Blood SugarFrom EverandGlucose Revolution: The Life-Changing Power of Balancing Your Blood SugarRating: 5 out of 5 stars5/5 (350)
- How to Be Well: The 6 Keys to a Happy and Healthy LifeFrom EverandHow to Be Well: The 6 Keys to a Happy and Healthy LifeRating: 5 out of 5 stars5/5 (1)
- Eat Complete: The 21 Nutrients That Fuel Brainpower, Boost Weight Loss, and Transform Your HealthFrom EverandEat Complete: The 21 Nutrients That Fuel Brainpower, Boost Weight Loss, and Transform Your HealthRating: 2 out of 5 stars2/5 (1)
- Eat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouFrom EverandEat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouNo ratings yet
- Grit & Grace: Train the Mind, Train the Body, Own Your LifeFrom EverandGrit & Grace: Train the Mind, Train the Body, Own Your LifeRating: 4 out of 5 stars4/5 (3)