You might also like
- RetainedplacentaDocument23 pagesRetainedplacentachindy layNo ratings yet
- Ob - Abnormalities of The Third Stage of Labor andDocument108 pagesOb - Abnormalities of The Third Stage of Labor andapi-3856051100% (2)
- 3rd Stage of LabourDocument10 pages3rd Stage of LabourBhawna JoshiNo ratings yet
- Third Stage of LaborDocument32 pagesThird Stage of LaborWhirmey ChinyamaNo ratings yet
- 35 - Retained PlacentaDocument11 pages35 - Retained Placentadr_asalehNo ratings yet
- LaborDocument2 pagesLaborclaritinNo ratings yet
- "Types of Abortion": A Reading ONDocument3 pages"Types of Abortion": A Reading ONJannine BensiNo ratings yet
- 3rd and 4th Stage of LabourDocument53 pages3rd and 4th Stage of LabourlisafelixNo ratings yet
- Retained PlacentaDocument30 pagesRetained PlacentaNejib M/AminNo ratings yet
- Abnormal Midwifery: Section 1: Multiple PregnanciesDocument104 pagesAbnormal Midwifery: Section 1: Multiple PregnanciesKelvinNo ratings yet
- 1066 Complications of 3rd Stage of Labour Injuries To Birth CanalDocument110 pages1066 Complications of 3rd Stage of Labour Injuries To Birth CanalSweety YadavNo ratings yet
- MCN ObDocument7 pagesMCN ObJoshua SaelNo ratings yet
- What Is Retained PlacentaDocument1 pageWhat Is Retained PlacentaKitkat Aquino CabugwasNo ratings yet
- Complication During Labor DeliveryDocument68 pagesComplication During Labor DeliveryJhennie Rose PalaganasNo ratings yet
- RetainedplacentaDocument14 pagesRetainedplacentachindy layNo ratings yet
- Active Management of Third Stage of LabourDocument27 pagesActive Management of Third Stage of LabourNagamalar RajendraNo ratings yet
- Postpartal ComplicationsDocument7 pagesPostpartal ComplicationsCeeNo ratings yet
- Fetal Dev, AbortionDocument128 pagesFetal Dev, AbortionAr JayNo ratings yet
- Normal Labour& Abnormal LabourDocument23 pagesNormal Labour& Abnormal LabourThetnaungsoe100% (1)
- Abnormaluterineaction 100515015711 Phpapp01Document40 pagesAbnormaluterineaction 100515015711 Phpapp01Seema Vashisht100% (1)
- Third Stage Complications and Post-Partum CollapseDocument44 pagesThird Stage Complications and Post-Partum CollapseRamlah Ibrahim100% (1)
- Dysfunctional Uterine ContractionDocument2 pagesDysfunctional Uterine ContractionAlphine DalgoNo ratings yet
- Complication During Labor DeliveryDocument68 pagesComplication During Labor DeliveryEllie ELLNo ratings yet
- Retained Placenta - Write UpDocument3 pagesRetained Placenta - Write UpGorgakilNo ratings yet
- Contraction Ring, Uterine Rupture, Precipitate LaborDocument4 pagesContraction Ring, Uterine Rupture, Precipitate LaborJessica Carmela CasugaNo ratings yet
- Stages of LabourDocument14 pagesStages of LabourSuriya KalaNo ratings yet
- What Is Retained PlacentaDocument7 pagesWhat Is Retained PlacentaA Xiao Yhing TrancoNo ratings yet
- Notes On The Complications During The Labor and Delivery ProcessDocument7 pagesNotes On The Complications During The Labor and Delivery ProcessjyzzadNo ratings yet
- AbortionDocument28 pagesAbortionlordgoncarNo ratings yet
- Labor and Delivery: By: Ma. Kizianne Krystel ManioDocument43 pagesLabor and Delivery: By: Ma. Kizianne Krystel ManioJohn Christian LasalitaNo ratings yet
- OBG 1stDocument24 pagesOBG 1stBhaskar PandeyNo ratings yet
- ABORTIONDocument2 pagesABORTIONRachel Nepomuceno HernandezNo ratings yet
- Retained PlacentaDocument15 pagesRetained PlacentagibreilNo ratings yet
- Types of Abortion FINALDocument2 pagesTypes of Abortion FINALAndrew_Ruiz_6140No ratings yet
- It Contains Highly Disturbing Graphical ContentDocument37 pagesIt Contains Highly Disturbing Graphical ContentErnest Jaberina VizcarraNo ratings yet
- Conyent Physiology of Third Stage of LabourDocument13 pagesConyent Physiology of Third Stage of LabourJay PaulNo ratings yet
- Power PointDocument21 pagesPower Point08chelleyNo ratings yet
- Abruptio PlacentaDocument4 pagesAbruptio PlacentaChelzie LasernaNo ratings yet
- MCN ReportDocument21 pagesMCN ReportJœnríčk AzueloNo ratings yet
- Complications During Labor and BirthDocument4 pagesComplications During Labor and BirthAudree Bustamante100% (2)
- Abnormal Uterine ActionDocument27 pagesAbnormal Uterine Actiontanmai noolu100% (1)
- Normal Labour in Obstetric2Document17 pagesNormal Labour in Obstetric2Tejasvi ChavdaNo ratings yet
- Retained PlacentaDocument2 pagesRetained PlacentaAmiraah MasriNo ratings yet
- NSVDDocument2 pagesNSVDBelleNo ratings yet
- Complications With The PowerDocument5 pagesComplications With The PowerHannrhey VelascoNo ratings yet
- Chapter 21: The Woman Who Develops A Complication During Labor and BirthDocument52 pagesChapter 21: The Woman Who Develops A Complication During Labor and BirthVincent Maralit MaterialNo ratings yet
- Placenta Accreta: What Is The Difference Between Accreta, Increta or Percreta?Document4 pagesPlacenta Accreta: What Is The Difference Between Accreta, Increta or Percreta?Bryan Neil GarmaNo ratings yet
- 3rd Stage of LaborDocument40 pages3rd Stage of Laborjeny patel100% (1)
- Manual Removal Retained Placenta - Sept18Document3 pagesManual Removal Retained Placenta - Sept18Chatrine Aprilia HendraswariNo ratings yet
- Mechanism of LabourDocument10 pagesMechanism of LabourMithlesh Dewangan100% (4)
- Ob REPORT PDFDocument44 pagesOb REPORT PDFJohn Michael SedanoNo ratings yet
- Actual Birth SimulationDocument47 pagesActual Birth SimulationBSN 1A- Serrano Evytte Joy B.No ratings yet
- High-Risks-Of-Pregnancies - JillDocument13 pagesHigh-Risks-Of-Pregnancies - JillMaureline DominarNo ratings yet
- A. Discuss The Four Stages of LaborDocument3 pagesA. Discuss The Four Stages of LaborAmoroso, Marian Corneth D.No ratings yet
- ACFrOgB40CYYfaqy K PEr1l2pQYS7J9CKoF1MzNRgUdEeaerp5y-GUUcxhhLpG-m5OUou-0hSVvKydlpjOQw2r0JNNDJa05hIf3kh47Kq6Qb3Lc4EbZZJrZnskvwOSk 94JNpKiPOaPE eXRxjIDocument6 pagesACFrOgB40CYYfaqy K PEr1l2pQYS7J9CKoF1MzNRgUdEeaerp5y-GUUcxhhLpG-m5OUou-0hSVvKydlpjOQw2r0JNNDJa05hIf3kh47Kq6Qb3Lc4EbZZJrZnskvwOSk 94JNpKiPOaPE eXRxjIJomer Levi PortuguezNo ratings yet
- Stages of LaborDocument3 pagesStages of LaborAmoroso, Marian Corneth D.No ratings yet
- Manual Removal Retained Placenta - Nov20Document3 pagesManual Removal Retained Placenta - Nov20Muhammad Raheel ShahNo ratings yet
- Abortion ProceduresDocument23 pagesAbortion ProceduresAjay JadejaNo ratings yet
- It's Not Just a Heavy Period; The Miscarriage HandbookFrom EverandIt's Not Just a Heavy Period; The Miscarriage HandbookRating: 2 out of 5 stars2/5 (1)
- Drug Study: Drug Name Dosage Indication Mechanism of Action Contraindication Side Effects Nursing ConsiderationDocument3 pagesDrug Study: Drug Name Dosage Indication Mechanism of Action Contraindication Side Effects Nursing ConsiderationRhea Jane BongcatoNo ratings yet
- Stages and Mechanism of LaborDocument14 pagesStages and Mechanism of LaborRhea Jane BongcatoNo ratings yet
- Chapter 36 and 37Document13 pagesChapter 36 and 37Rhea Jane BongcatoNo ratings yet
- Socio - Cultural AspectDocument19 pagesSocio - Cultural AspectRhea Jane BongcatoNo ratings yet
- Colonial PeriodDocument17 pagesColonial PeriodRhea Jane BongcatoNo ratings yet
- DRUG-STUDY PediaDocument5 pagesDRUG-STUDY PediaRhea Jane Bongcato50% (2)
- Resume Kantesh MundaragiDocument3 pagesResume Kantesh MundaragiKanteshNo ratings yet
- SHARE SEA Outlook Book 2518 r120719 2Document218 pagesSHARE SEA Outlook Book 2518 r120719 2Raafi SeiffNo ratings yet
- 5130 - 05 5G Industrial Applications and SolutionsDocument113 pages5130 - 05 5G Industrial Applications and SolutionsMauricio SantosNo ratings yet
- Technical ReportDocument39 pagesTechnical ReportTope-Akanni AyomideNo ratings yet
- MinimumEHS Standards For Projects-V3Document113 pagesMinimumEHS Standards For Projects-V3Ammu KuttiyNo ratings yet
- Knock Knock GamesDocument1 pageKnock Knock GamesArsyta AnandaNo ratings yet
- USMLE Step 2 CK Exam - Overview - Examination Content - Test Format - EligibilityDocument7 pagesUSMLE Step 2 CK Exam - Overview - Examination Content - Test Format - EligibilityJamesHowsonNo ratings yet
- Preparatory Surface Cleaning of Architectural Sandstone: Standard Practice ForDocument2 pagesPreparatory Surface Cleaning of Architectural Sandstone: Standard Practice Fors.swamyNo ratings yet
- Tolkien Essay-TreesDocument10 pagesTolkien Essay-Treesapi-657753727No ratings yet
- Nclex PogiDocument8 pagesNclex Pogijackyd5No ratings yet
- MMDA v. Viron Transportation CoDocument3 pagesMMDA v. Viron Transportation CoTtlrpqNo ratings yet
- APEX Forms Sergei MartensDocument17 pagesAPEX Forms Sergei MartensIPlayingGames 301No ratings yet
- Math9 - Q2 - Mod2 - WK 3 - JointAndCombinedVariations - Version2Document37 pagesMath9 - Q2 - Mod2 - WK 3 - JointAndCombinedVariations - Version2Precious Arni100% (7)
- Course Welcome and Overview ACADocument20 pagesCourse Welcome and Overview ACAAlmerNo ratings yet
- Downloaded From Manuals Search EngineDocument29 pagesDownloaded From Manuals Search EnginehaivermelosantanderNo ratings yet
- Leaders Eat Last Key PointsDocument8 pagesLeaders Eat Last Key Pointsfidoja100% (2)
- Natural Resources of Arunachal PradeshDocument7 pagesNatural Resources of Arunachal PradeshshivarathordiviyapurNo ratings yet
- M6 - Deductions P3 (13B) Students'Document56 pagesM6 - Deductions P3 (13B) Students'micaella pasionNo ratings yet
- A Psychological Crusade by Fernando Sorrentino - Text 7Document2 pagesA Psychological Crusade by Fernando Sorrentino - Text 7Donnie DominguezNo ratings yet
- Pineapple Working PaperDocument57 pagesPineapple Working PaperAnonymous EAineTiz100% (7)
- Ingles V Eje 1 Week 2Document5 pagesIngles V Eje 1 Week 2Cristhian Javier Torres PenaNo ratings yet
- Anthony D. Slonim, Murray M. Pollack Pediatric Critical Care Medicine PDFDocument950 pagesAnthony D. Slonim, Murray M. Pollack Pediatric Critical Care Medicine PDFAnca DumitruNo ratings yet
- Appraisal: Gilmore and Williams: Human Resource ManagementDocument18 pagesAppraisal: Gilmore and Williams: Human Resource ManagementShilpa GoreNo ratings yet
- List - of - Members As On 6 3 18 PDFDocument8 pagesList - of - Members As On 6 3 18 PDFashish jaiswal100% (1)
- SAmple Format (Police Report)Document3 pagesSAmple Format (Police Report)Johnpatrick DejesusNo ratings yet
- Synopsis On Employee LifecycleDocument12 pagesSynopsis On Employee LifecycleDeepak SinghNo ratings yet
- FAR MpsDocument2 pagesFAR MpsJENNIFER YBAÑEZNo ratings yet
- Exploration of MoonDocument8 pagesExploration of MoonAryan KhannaNo ratings yet
- Painter Decorator Curriculum Eng l1 2 3 CC 404c.404dDocument100 pagesPainter Decorator Curriculum Eng l1 2 3 CC 404c.404dM.a. KhaderNo ratings yet
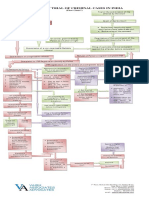
- Process of Trial of Criminal Cases in India (Flow Chart)Document1 pageProcess of Trial of Criminal Cases in India (Flow Chart)Arun Hiro100% (1)