You might also like
- 117cherished MomentsDocument32 pages117cherished MomentsPilar Martín Zamora100% (1)
- METABOLISM AND BIOTRANSFORMATION: AN OVERVIEWDocument33 pagesMETABOLISM AND BIOTRANSFORMATION: AN OVERVIEWAlphaRaj Mekapogu67% (3)
- Liver BiochemistryDocument30 pagesLiver BiochemistryIrina Cez100% (1)
- LEARNERS BOOK 1 (2) ... ScienceDocument160 pagesLEARNERS BOOK 1 (2) ... SciencehussamNo ratings yet
- Biochemical Response to XenobioticsDocument52 pagesBiochemical Response to XenobioticsTiaRa JuraidNo ratings yet
- Guided Reading Assessment The Giraffe Pelly and Me p19 38Document4 pagesGuided Reading Assessment The Giraffe Pelly and Me p19 38Joshua JamesNo ratings yet
- 10 - Bus 105 and 107-1Document400 pages10 - Bus 105 and 107-1Alao LateefNo ratings yet
- UNIT 2 ELIMINATION and BIOAVAILABILITY & BIOEQUIVALENCE PDFDocument207 pagesUNIT 2 ELIMINATION and BIOAVAILABILITY & BIOEQUIVALENCE PDFMamta Pant100% (4)
- Biotransformation and Excretion of DrugDocument63 pagesBiotransformation and Excretion of DrugIzzuddin AhmadNo ratings yet
- Assessment of Metabolic AcidosisDocument34 pagesAssessment of Metabolic Acidosisfatha100% (1)
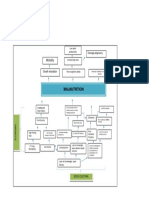
- Problem Tree Analysis MalnutritionDocument1 pageProblem Tree Analysis MalnutritionMho Dsb50% (6)
- Environmental Sustainability Assessment of An Academic Institution in Calamba CityDocument29 pagesEnvironmental Sustainability Assessment of An Academic Institution in Calamba CityAmadeus Fernando M. PagenteNo ratings yet
- Sell More, Serve BetterDocument39 pagesSell More, Serve BetterSalesMantra CRM100% (4)
- Xenobiotics and Its Metabolism: Group 7Document31 pagesXenobiotics and Its Metabolism: Group 7markganir08No ratings yet
- BiotransformationDocument34 pagesBiotransformationDinda saylaNo ratings yet
- Bio Chem EssaysDocument20 pagesBio Chem EssaysEINSTEIN2DNo ratings yet
- Phase: I Hydrolysis of XenobioticsDocument37 pagesPhase: I Hydrolysis of XenobioticsSunilNo ratings yet
- Lecture 4 Metabolism Phase Iv 2Document49 pagesLecture 4 Metabolism Phase Iv 2Umar AzadNo ratings yet
- Metabolism 2017Document96 pagesMetabolism 2017aimaNo ratings yet
- Basic ConceptsDocument38 pagesBasic ConceptsSneha PatilNo ratings yet
- Lecture 2 Drug Metabolism Phase IIDocument27 pagesLecture 2 Drug Metabolism Phase IIfeegame7No ratings yet
- 1 - Biochemistry Notes by Dr. M A Bari Siddiqui: DrmentorsDocument3 pages1 - Biochemistry Notes by Dr. M A Bari Siddiqui: DrmentorsShiva KumarNo ratings yet
- Xenobiotics MetabolismDocument47 pagesXenobiotics Metabolismademabdella38No ratings yet
- Biochemistry of Xenobiotic Metabolism in the LiverDocument3 pagesBiochemistry of Xenobiotic Metabolism in the LiverjimmyNo ratings yet
- Biotransformation SeminarDocument16 pagesBiotransformation SeminarShreyasNo ratings yet
- Metabolism of XenobioticsDocument54 pagesMetabolism of XenobioticsAurellia ShafitriNo ratings yet
- METABOLISM OF XENOBIOTICS-revDocument28 pagesMETABOLISM OF XENOBIOTICS-revEdo Pramana PutraNo ratings yet
- XENOBi OTIKDocument70 pagesXENOBi OTIKLie FelixNo ratings yet
- Liver's role in detoxifying xenobiotics and endogenous toxinsDocument34 pagesLiver's role in detoxifying xenobiotics and endogenous toxinsМохіт Кумар ЯмпатіNo ratings yet
- Alcoholism Fatty Liver Liver Cirrhosisg6b1Document48 pagesAlcoholism Fatty Liver Liver Cirrhosisg6b1Franc SalinasNo ratings yet
- Metabolism of Xenobiotics: A Concise OverviewDocument23 pagesMetabolism of Xenobiotics: A Concise OverviewNayana Ranjan FranandoNo ratings yet
- BCH 220 - DR ErhunseDocument6 pagesBCH 220 - DR ErhunseSuccess OlamideNo ratings yet
- Kuliah Farmakokinetik Metabolisme Obat 10 Mei 2010Document78 pagesKuliah Farmakokinetik Metabolisme Obat 10 Mei 2010SALSABILA RAHMA REFFANANANo ratings yet
- Role of Free Radicals in Health and DiseaseDocument49 pagesRole of Free Radicals in Health and DiseaseKuzhandai VeluNo ratings yet
- BiochemistryDocument33 pagesBiochemistryamhhospital0No ratings yet
- Metabolism of Xenobiotics: A Three Phase ProcessDocument84 pagesMetabolism of Xenobiotics: A Three Phase ProcessJNo ratings yet
- 1 - XenobioticsDocument24 pages1 - XenobioticsgeenaksamuelNo ratings yet
- Xenobiotic MetabolismDocument64 pagesXenobiotic MetabolismBelajar dan berdoaNo ratings yet
- Drug MetabolismDocument52 pagesDrug MetabolismUsman AkhtarNo ratings yet
- 04 Metabolisme Xenobiotik NWDocument36 pages04 Metabolisme Xenobiotik NWDesy NataliaNo ratings yet
- Acid Base DisordersDocument51 pagesAcid Base Disordersmmkavitha98No ratings yet
- Xenobiotic Metabolism PDFDocument50 pagesXenobiotic Metabolism PDFroxy8marie8chanNo ratings yet
- Xenobiotic FKBiotransformationDocument100 pagesXenobiotic FKBiotransformationMuhammad SyaifullahNo ratings yet
- Metabolism of XenobioticsDocument30 pagesMetabolism of XenobioticsCzarina RiveraNo ratings yet
- Uronic Acid Pathway and HMP PathwayDocument3 pagesUronic Acid Pathway and HMP PathwaykanhaNo ratings yet
- HyperuricemiaDocument10 pagesHyperuricemianinroseNo ratings yet
- Xenobiotics MetabolismDocument4 pagesXenobiotics MetabolismMohammed L BalloNo ratings yet
- The Patient With Metabolic Alkalosis: October 2018Document9 pagesThe Patient With Metabolic Alkalosis: October 2018NirmalaNo ratings yet
- Water: PH and BuffersDocument63 pagesWater: PH and BuffersSoffa ShmuelNo ratings yet
- Drug Affecting Metabolism by RinkuDocument23 pagesDrug Affecting Metabolism by RinkuRinku KunduNo ratings yet
- Lecture 13. Xenobiotics Phases and Mechanisms of Biotransformation, The Role of Cytochrome P450Document15 pagesLecture 13. Xenobiotics Phases and Mechanisms of Biotransformation, The Role of Cytochrome P450Віталій Михайлович НечипорукNo ratings yet
- Drug Metabolism: Phase I and Phase II Metabolism: Principal Organs For BiotransformationDocument9 pagesDrug Metabolism: Phase I and Phase II Metabolism: Principal Organs For Biotransformationdavid5king-3119No ratings yet
- PorfirinDocument27 pagesPorfirinwulandewi1512No ratings yet
- BCH421 2019-20 Harmattan 1Document7 pagesBCH421 2019-20 Harmattan 1idriscognitoleadsNo ratings yet
- Drug MetabolismDocument43 pagesDrug MetabolismKelly PatrickNo ratings yet
- Biochemical Functions of The LiverDocument25 pagesBiochemical Functions of The LiverSaifNo ratings yet
- Sharkey 2015Document11 pagesSharkey 2015Mauricio MedinaNo ratings yet
- Detect Lactic Acidosis EarlyDocument27 pagesDetect Lactic Acidosis Earlydragab71No ratings yet
- Metabolism or Biotransformation of Drugs in The BodyDocument84 pagesMetabolism or Biotransformation of Drugs in The BodyDhruv RanaNo ratings yet
- LECTURE 4 - Major Intra - and Extracellular ElectrolytesDocument66 pagesLECTURE 4 - Major Intra - and Extracellular ElectrolytesGamotkoto PharmacyNo ratings yet
- DRUG MTABOLISM-1Document79 pagesDRUG MTABOLISM-1Ebenezer SamuelNo ratings yet
- Drug MetabolismDocument43 pagesDrug MetabolismAinsleyNo ratings yet
- Understanding Acid-Base BalanceDocument3 pagesUnderstanding Acid-Base Balanceabxaz100% (1)
- CHAPTER 5 MetabolismeDocument46 pagesCHAPTER 5 MetabolismeYuli Irvaransiah DIatun NIkmahNo ratings yet
- Drug Metabolism and Excretion: An OverviewDocument19 pagesDrug Metabolism and Excretion: An OverviewAsadullah ghalibNo ratings yet
- Cover Letter and Thank You Letter ExamplesDocument7 pagesCover Letter and Thank You Letter Examplesf675ztsf100% (2)
- Prediction of Hospital Admission Using Machine LearningDocument9 pagesPrediction of Hospital Admission Using Machine LearningTRIAD TECHNO SERVICESNo ratings yet
- Hesi v2Document125 pagesHesi v2kandiezein88No ratings yet
- Kinematics of MachineDocument4 pagesKinematics of MachineSumit KambleNo ratings yet
- Minutes of Meeting 12-09-17Document3 pagesMinutes of Meeting 12-09-17MykaNo ratings yet
- FSLDMDocument5 pagesFSLDMaiabbasi9615No ratings yet
- Unit Gandhbsm and Pacifism: N Global Village. However, The World Is Swept by TlicDocument9 pagesUnit Gandhbsm and Pacifism: N Global Village. However, The World Is Swept by TlicArjun KSNo ratings yet
- Explicitation and Implicitation - Omission and Addition - in ENGLISHDocument63 pagesExplicitation and Implicitation - Omission and Addition - in ENGLISHdyna bookNo ratings yet
- 562ue 2014-06Document55 pages562ue 2014-06vijayramaswamyNo ratings yet
- The Lair of Arachas - A Mausritter AdventureDocument8 pagesThe Lair of Arachas - A Mausritter AdventureGladstone PinheiroNo ratings yet
- DinithDocument102 pagesDinithVishmi amashaNo ratings yet
- ReportDocument3 pagesReportPrecious Anne MacalinoNo ratings yet
- Effectiveness of Workplace Counseling On Employee Performance. A Case of Mumias Sugar Company Limited, KenyaDocument10 pagesEffectiveness of Workplace Counseling On Employee Performance. A Case of Mumias Sugar Company Limited, KenyainventionjournalsNo ratings yet
- Operations Management Service ExcellenceDocument18 pagesOperations Management Service ExcellenceParth PatelNo ratings yet
- Dokumen - Tips - Ielts and Toefl Made Easy George John Efc and Is The First Coherence PDFDocument2 pagesDokumen - Tips - Ielts and Toefl Made Easy George John Efc and Is The First Coherence PDFPayal SethiNo ratings yet
- English Revision Notes XIIDocument41 pagesEnglish Revision Notes XIIRämíz MêmóñNo ratings yet
- Okhistorych 9 NotesDocument18 pagesOkhistorych 9 Notesapi-337913436No ratings yet
- Notes For MDES PsychologyDocument31 pagesNotes For MDES Psychologyvct64677No ratings yet
- Pon Vidyashram Group of Cbse Schools STD 8 SCIENCE NOTES (2020-2021)Document3 pagesPon Vidyashram Group of Cbse Schools STD 8 SCIENCE NOTES (2020-2021)Bharath Kumar 041No ratings yet
- Holistic Retreat, Doi Saket, Chiang MaiDocument4 pagesHolistic Retreat, Doi Saket, Chiang MaiShireenNo ratings yet
- Strict Liability Offences ExplainedDocument7 pagesStrict Liability Offences ExplainedJoseph ClarkNo ratings yet
- Beed III-lesson 1.1-The Curricula in School Sept 4 2021Document7 pagesBeed III-lesson 1.1-The Curricula in School Sept 4 2021catherine r. apusagaNo ratings yet
- Income Tax and GST PDFDocument152 pagesIncome Tax and GST PDFAdharsh EsNo ratings yet