You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Production, Regulation, and Action of Thyroid HormonesDocument51 pagesProduction, Regulation, and Action of Thyroid HormonesNona AsolaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- The Endocrine Pancreas: Regulation of Carbohydrate MetabolismDocument61 pagesThe Endocrine Pancreas: Regulation of Carbohydrate MetabolismNona AsolaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Nervous Sys. 7Document30 pagesNervous Sys. 7Nona AsolaNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Muscle Phys, TCA, Krebs, Catabolism V1.2Document21 pagesMuscle Phys, TCA, Krebs, Catabolism V1.2Nona AsolaNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Bio DefinitionsDocument22 pagesBio Definitions青木ケイNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Protocols For High-Risk Pregnancies - 2010 - Queenan - Appendix B Laboratory Values in Normal PregnancyDocument9 pagesProtocols For High-Risk Pregnancies - 2010 - Queenan - Appendix B Laboratory Values in Normal PregnancyHenry VillarosaNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Chapter 39: Hematologic Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionDocument5 pagesChapter 39: Hematologic Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionHelen UgochukwuNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Glasgow-Blatchford Score - WikipediaDocument10 pagesGlasgow-Blatchford Score - Wikipediaaamir afridiNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- 02 - CLS 382 - 443 - ProteinDocument21 pages02 - CLS 382 - 443 - ProteinamalNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- GANOTHERAPY - The Holistic Health TherapyDocument3 pagesGANOTHERAPY - The Holistic Health TherapyThe Enthusiast100% (2)
- BB Ans 1 PDFDocument6 pagesBB Ans 1 PDFAnne MorenoNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- HRM Week 2 - Introduction 2020 - PrintDocument34 pagesHRM Week 2 - Introduction 2020 - PrintShiv SookunNo ratings yet
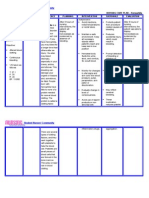
- NURSING CARE PLAN - HemophiliaDocument2 pagesNURSING CARE PLAN - Hemophiliaderic91% (11)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 101 Modul Hebat Bio 2021 - PDF - Eng-47-55Document9 pages101 Modul Hebat Bio 2021 - PDF - Eng-47-55BF CLNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Human Respiratory SystemDocument13 pagesHuman Respiratory SystemKarma DemaNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Biochemical Markers For Clinical Monitoring of Tissue PerfusionDocument14 pagesBiochemical Markers For Clinical Monitoring of Tissue PerfusionTrọng MPNo ratings yet
- Mohit CBC 18Document1 pageMohit CBC 18amit2352842No ratings yet
- Plasma: Ifcc Transport Storage BloodDocument6 pagesPlasma: Ifcc Transport Storage BloodFalanta SandaNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- HemophiliaDocument60 pagesHemophiliavibhurocksNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- 038 Health In1 PDFDocument281 pages038 Health In1 PDFbhatchinmay7100% (1)
- Experiment No.6 Blood Grouping and Blood Typing Objective: Materials: ProcedureDocument3 pagesExperiment No.6 Blood Grouping and Blood Typing Objective: Materials: ProcedureClaveria Jeric FernandezNo ratings yet
- Slide Kuliah Transfusi DarahDocument31 pagesSlide Kuliah Transfusi Darahfenti nurul khafifahNo ratings yet
- Para Protein Emi ADocument14 pagesPara Protein Emi AMohamoud MohamedNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Science 9 Week 1Document18 pagesScience 9 Week 1lenNo ratings yet
- Science Grade 7 Second QuarterDocument12 pagesScience Grade 7 Second QuarterAnneKARYLE67% (3)
- Hypertension and Congestive Heart FailureDocument4 pagesHypertension and Congestive Heart FailureDawn ReyaNo ratings yet
- Lecture 13 Blood 1Document19 pagesLecture 13 Blood 1Sufian ShahidNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- HemorrhageDocument13 pagesHemorrhagekins.bhojaniNo ratings yet
- ICSH Guidance For Coagulation Critical Values and TestsDocument51 pagesICSH Guidance For Coagulation Critical Values and Testscitometria prolabNo ratings yet
- Life Sciences Grade 10 ATP 2024Document19 pagesLife Sciences Grade 10 ATP 2024olwe149No ratings yet
- 1 s2.0 S0887796318300853 Main PDFDocument8 pages1 s2.0 S0887796318300853 Main PDFOncología CdsNo ratings yet
- Nandini SpouseDocument10 pagesNandini SpouseGanesh GaniNo ratings yet
- Edexcel International GCSE Biology Workbook Erica Larkcom, RogerDocument97 pagesEdexcel International GCSE Biology Workbook Erica Larkcom, RogerLa Won Yan100% (1)
- Suggested Answers To Practical Workbook: CH 7 Gas Exchange in HumansDocument31 pagesSuggested Answers To Practical Workbook: CH 7 Gas Exchange in HumansCharmine HolmesNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)